

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The nasal cavity is connected to the bronchus by a single airway passage, and rhinitis is frequently associated with co-morbidities like asthma, which suggests the concept "one airway one disease". The implication of this is that rhinitis and such co-morbidities are manifestations of one disease process which affects different parts of the airway [1-3].
Chronic rhinitis is a heterogeneous group of upper airway diseases [4], which can be classified according to the presence of atopy or nasal polyposis. Chronic rhinosinusitis with nasal polyps (CRSwNP) is characterized by a T-helper-2 dominated cytokine pattern in nasal mucosa, whereas chronic rhinosinusitis without polyps (CRSsNP), exhibits T-helper-1 biased cytokine release [5]. In addition, chronic rhinitis can also be classified as allergic rhinitis (AR) or non-allergic rhinitis (NAR) based on the presence or absence of atopy, which is determined by systemic atopy test such as skin prick test or in vitro test for antigen-specific IgE in serum. However, recent studies reported that AR and NAR are associated with similar local IgE-induced inflammation in nasal mucosa regardless of systemic atopy test findings [6, 7]. Rondón et al. [8] even suggested that, in adults, NAR can switch to become AR with asthma, conjunctivitis, or both with aeroallergen sensitization at a later date.
We hypothesized that there could be differences between the different forms of chronic rhinitis in terms of lower airway inflammation and evaluated the differences in lower airway inf lammation among dif ferent forms of chronic rhinitis according to the presence of atopy, nasal polyposis or airway hyperresponsiveness. Lower airway inflammation was evaluated by inducing sputum, which contains constituents of respiratory epithelium, mainly from the central airways [9]. The mRNA levels of IL-5, IFN-γ, TGF-β1, IL-17A1, and IL-25 in induced sputum samples were measured using quantitative real-time PCR. IL-5, IFN-γ and TGF-β1 are known to be significant different in nasal inflammation between CRSwNP and CRSsNP, and IL-17A1 increased in nasal polyps in Asian patients in recent studies [10].
Go to : 
MATERIALS AND METHODS
Study subjects
Of the patients that attended the allergy outpatient clinic at Seoul National University Hospital between January 2007 and April 2009, those that presented with moderate/severe persistent rhinitis symptoms (more than three among the following; frequent sneezing, itchy nose, watery rhinorrhea and nasal obstruction) for more than 1 year were enrolled [11]. The medical records were reviewed retrospectively. These included rhinoscopy, methacholine bronchial provocation test (MBPT), differential cell counts in induced sputum, and systemic atopy test (the skin prick test or the multiple allergosorbent test [MAST]).
The patients with chronic rhinitis were classified into two groups (house dust mites (HDM)-sensitive AR or NAR) according to the presence of atopy, and additionally according to nasal polyposis and airway hyperresponsiveness, respectively. The patients sensitive to other allergens except HDM (D. pteronyssinus, D. farinae), mostly seasonal allergens, were excluded because the inflammation and cell profiles of induced sputum in such patients could be highly variable according to the season when induced sputum was examined. So following patients were excluded: those sensitive to other allergens except HDM, those with a smoking history, and those treated with systemic or inhaled corticosteroids except nasal corticosteroids. Non-atopy was defined as none of positive response in the skin prick test with 55 common inhalant allergens (positive response: a wheal diameter of allergen ÷ wheal diameter of histamine of ≥1 and a mean wheal size ≥3 mm) or in MAST (Hitachi Chemical Diagnostics, Inc., Mountain View, CA, USA) of inhalant panel (more than class 2 MAST value to one of the allergens) [12, 13]. The mRNA levels of IL-5, IFN-γ, TGF-β1, IL-17A and IL-25 were evaluated in induced sputum samples by quantitative real-time RT-PCR. The enrolled patients with chronic rhinitis were divided into two groups according to the presence of atopy, nasal polyposis, and airway hypersensitivity, respectively. Nasal polyposis was diagnosed based on serial rhinoscopy. Airway hyperresponsiveness was defined by positive in MBPT. The study protocol was approved by the Institutional Review Board of Seoul National University Hospital (No. 1001-057-307).
Procedures
Skin prick tests were performed using test kit that included a battery of 55 common inhalant allergens (Allergopharma Co., Reinbek, Germany), a positive control (histamine 1 mg/mL) and negative diluent controls (Allergopharma Co.) [13]. MBPT was performed as previously described [14]. Medication such as antihistamine and leukotriene modifiers was discontinued at least 1 week before the test. Positive MBPT was defined by ≤16 mg/mL of the concentration of methacholine that induced >20% fall in forced expiratory volume in 1 sec (FEV1). Sputum induction and processing was performed as previously described [15].
Sputum induction and processing
Sputum induction was performed as previously described [15]. "After pretreatment with 400 µg inhaled salbutamol (Ventolin™, GlaxoSmithKline, Brentford, UK), 4.5% hypertonic saline was administered using an ultrasonic nebulizer at 4.5 mL/min (Omron Co., Tokyo, Japan), and repeated up to four times at 5 min intervals unless >10% fall in FEV1 occurred, in which induction procedure was stopped." And then sputum processing was performed as previously described [15]. "A freshly prepared dithiothreitol (DTE, 0.01 M) was added to sputum samples, which was then vortex mixed and shaken for 20 min at room temperature, filtered through a 52 mm nylon gauze to remove debris and mucus, and then centrifuged at 450 g for 10 min. Cell pellets obtained were resuspended in phosphate buffer saline to a volume equal to the original sputum plus DTE. Total cell counting was carried out using a hemocytometer and cell concentrations were then adjusted to 1.0 × 106 cells/mL. Cytospins were prepared by adding 60 µL of this cell suspension to Shandon II cytocentrifuge cups (Shandon Southern Instruments, Sewickley, PA, USA) and spun for 5 min at 500 rpm. Slides were stained with Diff-Quik solution (Sysmex Co., Kobe, Japan) to obtain differential leukocyte, bronchial epithelial cell, and squamous cell counts. To quantify cell differentiation, 300 nucleated cells per slide were counted and these counts were expressed as percentages of the number of intact round nucleated cells (excluding squamous epithelial cells) present. Sputum samples that contained more than 20% squamous epithelial cells were not analyzed."
RNA extraction and reverse transcription-PCR
Cells were isolated by brief centrifugation and then stored in 1 mL Trizol (Gibco, Carlsbad, CA, USA) at -80℃ until required. RNA was extracted by phenol/chloroform extraction and ethanol precipitation according to the manufacturer's instructions. RNA levels were determined spectrophotometrically (Nanodrop ND-1000, Wilmington, DE, USA) and 2 µg of RNA from each sample was reverse transcribed into cDNA using a single-strand cDNA synthesis kit (Promega Co., Madison, WI, USA).
Cytokine expressions in sputum cells by real-time quantitative PCR
Quantitative real-time PCR was performed on a 7500 Real-time PCR System (Applied Biosystems, Foster, CA, USA). The mRNA expressions of cytokines were determined by real-time PCR using a SYBR Green Master Mix (Applied Biosystems). Thermocycler conditions involved an initial holding period at 50℃ for 2 min and a sec holding period at 95℃ for 10 min, which was followed by a 2-step PCR program at 95℃ for 15 sec and 60℃ for 60 sec for 40 cycles. Data were collected and quantitatively analyzed on an ABI Prism 7500 Sequence Detection System (Applied Biosystems, Foster, CA, USA). The β2m gene was used as an endogenous control for sample normalization. Results are presented as fold values relative to β2m expression. The sequences of PCR primer pairs used were as follows: human β2m, forward 5'-CCAGCAGAGAATGGAAAGTC-3' and reverse 5'-GATGCTGCTTACATGTCTCG-3'; human IL-17A, forward 5'-AAACAACGATGACTCCTGGG-3' and reverse 5'-GAGGACCTTTTGGGATTGGT-3'; human IL-5, forward 5'-AGGAGCCGCAAGCTAAAAGC-3' and reverse 5'-TGCCTTCGTGCCCACTGT-3'; human TGF-β1, forward 5'-CCCAGCATCTGCAAAGCTC-3' and reverse 5'-GTCAATGTACAGCTGCCGCA-3'.
Statistical analysis
The data were analyzed using Pearson's chi-square test or the Mann-Whitney test in the SPSS ver. 12.0 for Windows software package (SPSS Inc., Chicago, IL, USA). Statistical significance was accepted for p values of < 0.05.
Go to :
RESULTS
There were 146 patients with moderate to severe persistent rhinitis symptoms. However, 60 patients with a history of smoking, 13 patients sensitive to seasonal allergens, and 8 patients without atopy or MBPT results were excluded. Finally, 65 patients were enrolled in this study, and induced sputum samples from 53 patients were evaluated for cytokine mRNA levels.
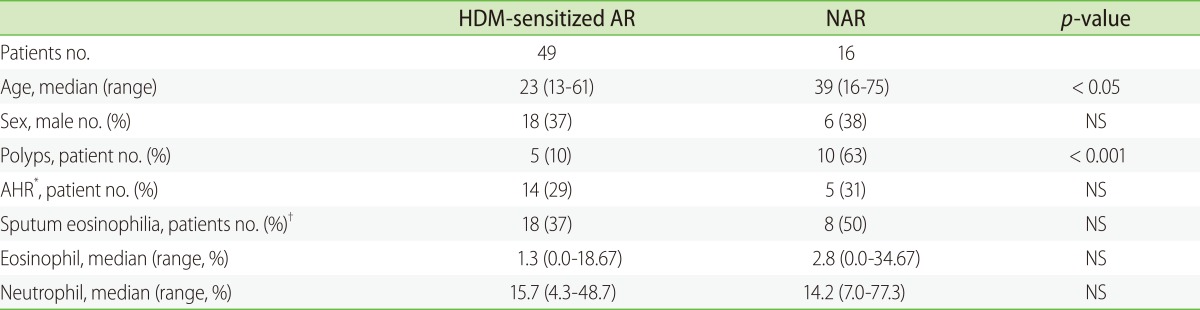
NAR patients were older than HDM-sensitized AR patients (39 [16-75] vs. 23 [13-61] years [medians (ranges)]; p < 0.05) and nasal polyposis was more common in NAR patients (10.2% vs. 62.5%, p < 0.001). However, no differences were observed between NAR and HDM-sensitized AR patients with respect to induced sputum cell profiles or the frequency of airway hyperresponsiveness (Table 1). NAR patients were found to have significantly higher IL-17A mRNA levels in the induced sputum (p = 0.016). Even after excluding patients with airway hyperresponsiveness, IL-17A mRNA levels were higher in NAR patients. However, no differences in IL-5, IFN-γ, TGF-β1, or IL-25 levels were found between the two groups (Fig. 1).
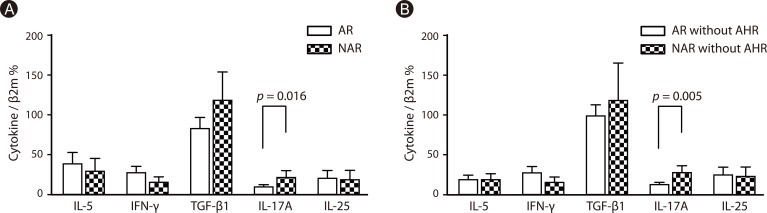 | Fig. 1Cytokine mRNA in the induced sputum samples of HDM-sensitized AR and NAR patients. (A) HDM-sensitized AR patients (n = 45) and NAR patients (n = 8). (B) HDM-sensitized AR patients without AHR (n = 31) and NAR patients without AHR (n = 6).
HDM, house dust mites; AR, allergic rhinitis; NAR, non-allergic rhinitis; AHR, airway hyperresponsiveness (PC20 ≤16 mg/mL).
|
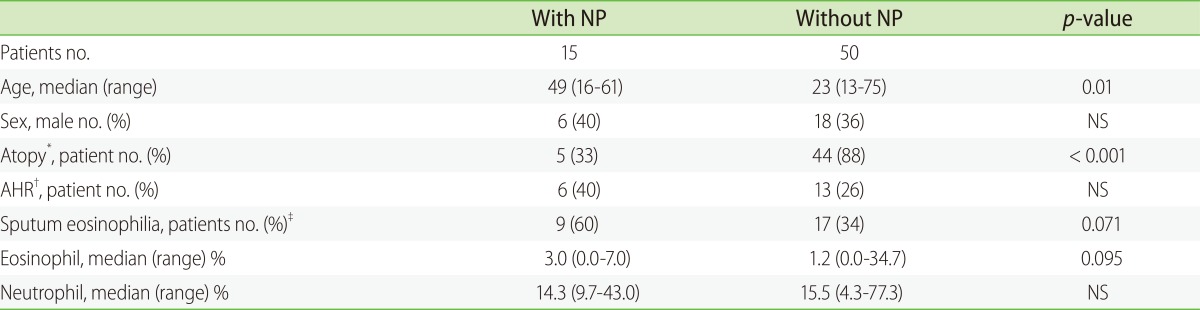
In terms of nasal polyposis, patients with nasal polyposis were significantly younger than patients without nasal polyposis (p = 0.01). The rate of atopy was greater among the patients without nasal polyposis (p < 0.001). No significant difference was observed between these two groups in terms of induced sputum cell profiles or the rate of airway hyperresponsiveness (Table 2). Though there were marginal differences in IL-5 mRNA expression levels between two groups in induced sputum (p = 0.052), no significant differences were found for the mRNA expression levels of IL-5, IFN-γ TGF-β1, IL-25, or IL-17A between two groups (Fig. 2).
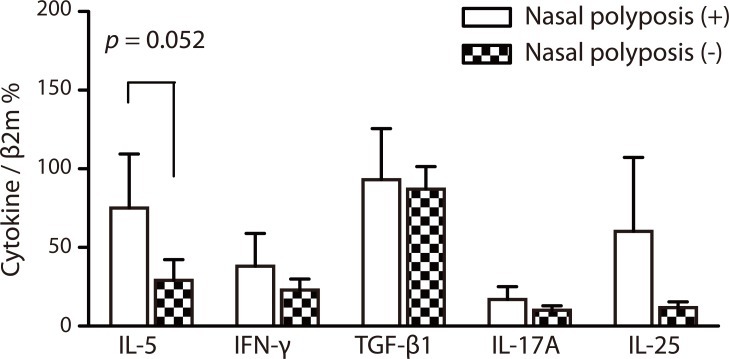 | Fig. 2Cytokine mRNA in the induced sputum samples according to the presence of nasal polyposis. Induced sputum samples were evaluated in chronic rhinitis patients with nasal polyposis (n = 9) and without nasal polyposis (n = 44). Nasal polyposis (+), chronic rhinitis with nasal polyposis. Nasal polyposis (-), chronic rhinitis without nasal polyposis.
|
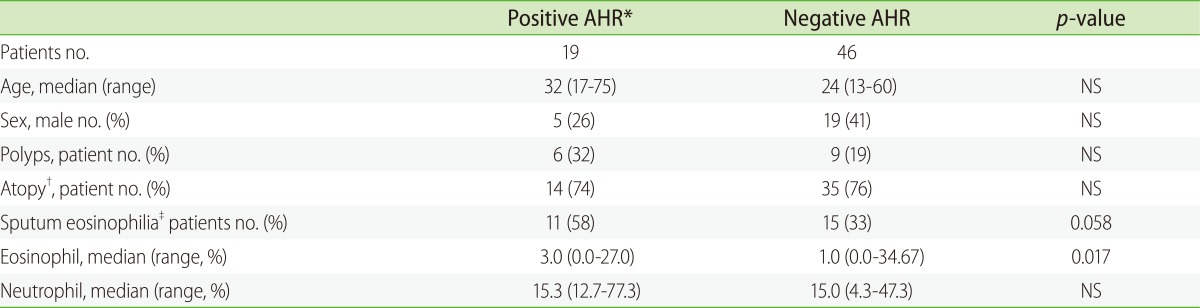
The induced sputum eosinophil ratio and the expression level of IL-5 mRNA in induced sputum were found to be higher in patients with airway hyperresponsiveness (p = 0.004 and p = 0.017, respectively; Table 3, Fig. 3). However, age, sex, atopy, the frequency of nasal polyposis, and the mRNA expression levels of IFN-γ TGF-β1, IL-25 and IL-17A were similar in patients with/without airway hyperresponsiveness.

Go to :
DISCUSSION
In this study, among the patients with moderate to severe persistent rhinitis symptoms, the expression level of IL-17A mRNA in the induced sputum was higher in NAR patients than HDM-sensitized AR patients (p = 0.016). This suggests that NAR patients have some degree of bronchial inflammation which is related to the elevated expression of IL-17A, and AR patients and NAR patients may have different inflammatory environments in their lower airway.
Several previous studies have addressed the differences between AR and NAR in a clinical setting, and then reported that the patients with AR have more sneezing and nasal pruritus, whereas the patients with NAR were characterized mainly by nasal obstruction and rhinorrhea [16, 17]. Comorbidities also differed in NAR and AR. Patients with NAR suffered more from sinusitis, whereas patients with AR suffer more frequently from conjunctivitis [16]. However, in the aspects of nasal inflammation, recent studies suggest that AR and NAR are associated with similar local IgE-induced inflammation in nasal mucosa regardless of systemic atopy test findings [6, 7]. Rondón et al. [6] reported 54% of patients with persistent NAR had a positive nasal allergen provocation test result to D. pteronyssinus and 22% had nasal specific IgE to D. pteronyssinus. The demonstration of IL-4 mRNA and germline epsilon gene transcripts in nasal mucosa following nasal allergen provocation suggest the potential for local immunoglobulin class switching following nasal mucosa exposure to antigen [18]. Thus many studies have concluded that local tissue IgE might specifically reflect true allergic status [8, 19]. In the connection with lower airway inflammation, rhinitis is found to be a risk factor of asthma regardless of atopic state [3, 20]. Several studies reported that similar inflammatory cells are present not only in the airways of patients with asthma but also in airways of nonasthmatic patients with AR, and even in the airways of atopic nonasthmtics without rhinitis [21-24]. Semik-Orzech et al. [25] reported that nasal allergen challenge induces the enhanced secretion of IL-17 and RANTES in the lower airways of nonasthmatic patients with AR. However little is known about NAR in terms of lower airway inflammation.
Present study suggests that there is relative IL-17A dominant inflammation in bronchial airway in NAR patients compared to HDM-sensitized AR patients. Our findings also suggest that in the patients with chronic rhinitis, different findings in systemic atopy test could mean differences in the central airway inflammation, which hints that the mechanisms responsible for local IgE inflammation in AR and NAR differ. IL-17 is a profibrotic cytokine that is associated with subepithelial fibrosis and may play a role in the remodeling of the nasal airways regardless of atopic state [26, 27]. IL-17 is also suspected to do pivotal role in the regulation of Th2 mediated allergic responses and might be a marker of allergy severity in AR [26, 28-31]. IL-17 is related to nasal polyposis and the elevation of IL-17 is associated with asthma [4, 20, 32]. The reason why the expression levels of IL-17 in severe AR, nasal polyps, or asthma are elevated has not been determined [20, 32-35]. However, several studies suggested that Staphylococcus aureus enterotoxin (SAE) could be one of possible causes [5, 36]. SAE causes local Th2 inflammation by acting as a super antigen and superantigenic S. aureus is particularly efficient at stimulating IL-17 production by memory T cells [37]. So SAE could be a possible cause of NAR or non-allergic asthma [35], and might explain the mechanisms responsible for local IgE inflammation in NAR and IL-17 dominant inflammation in lower airway of NAR patients.
Several important limitations of this study should be mentioned. First, the study was performed retrospectively, and thus, nasal polyp and mucosal tissues could not be evaluated and data on asthma symptoms were not available. Second, the ages of patients in each group were significantly different and the number of enrolled patients, particularly, the number of NAR patients was relatively small. In addition, no healthy control group was enrolled. However, in spite of these limitations, there are several findings in this study which are entirely consistent with the results of previous studies; nasal polyps were more common in NAR patients than in AR patients, and the sputum eosinophilia and the elevated level of IL-5 mRNA in patients with airway hyperresponsiveness [4, 15, 38].
This study suggests that NAR and AR especially sensitized to HDM may have different forms of inflammation in their lower airways in the patients with moderate to severe persistent rhinitis symptoms, and NAR patients have bronchial inflammation which is related to the elevated level of IL-17A. Although further studies are needed to determine the pathophysiologic differences in lower airways of AR and NAR, this study is the first to evaluate differences between AR and NAR in terms of lower airway inflammation. Evaluations for the heterogeneous nature of chronic rhinitis in relation to lower airway inflammation could be useful to understand the heterogeneous characters of lower airway inflammations by chronic diseases such as asthma and COPD.
Go to :
 XML Download
XML Download