

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Rhinitis is an inflammation of the upper airways that is characterised by symptoms of runny (rhinorrhea) and/or blocked nose and/or sneezing occurring for two or more consecutive days and lasting for more than an hour for most days [1, 2]. The Allergic Rhinitis and its Impact on Asthma (ARIA) guideline classifies rhinitis into allergic rhinitis (AR) and non-allergic rhinitis (NAR) based on the presence and absence of allergic sensitization. AR arises due to IgE-mediated mechanisms and is usually characterized with additional symptoms of itchy eyes (conjunctivitis). NAR has multiple possible triggers including infectious, hormonal, occupational, and idiopathic (previously termed as vasomotor rhinitis) [2]. It could well be that rhinitis in young children would involve both components of AR and NAR.
Rhinitis has been trivialized by clinicians as it does not cause fatalities, and has been understudied. More recently, however, rhinitis has been recognized to impose significant morbidity and has a significant impact on the quality of life. It is in fact now considered a considerable global medical burden with a significant economical cost [2]. A recent paediatric survey of children 4-17 years old conducted in the United States showed that rhinitis affects the quality of life (work and sleep) of sufferers and their caregivers [3]. Aside from the direct cost of rhinitis medications, rhinitis also exerts an indirect cost through its co-morbidities such as asthma. An example of this was illustrated by a study by Kang et al that rhinitis in children increased the number of outpatient and hospital visits of asthma sufferers [4].
Two birth cohort studies monitoring the natural history of childhood rhinitis [5, 6] showed a trend of increasing prevalence over time from infancy to adolescents. In these studies, symptoms of rhinitis were already observable from preschool age. Various others studies had also shown that rhinitis symptoms are already prevalent in the first 6 years of life. Except for these studies, it is our impression that rhinitis in early childhood is poorly characterised.
This review aims to summarize our current knowledge and to discuss the gaps in knowledge regarding AR in early childhood.
Methods
Literature search was conducted using a PubMed search with the following key terms: 'rhinitis' and 'preschool', and filtering for articles in English and published 2006-2011 (n = 565 articles). We screen titles and abstracts of the search results for studies discussing rhinitis separate from other morbidities, and also for studies discussing subjects <6 years old separately from older children. The screened publications were selected based on the following criteria: (1) Epidemiology and risk factor analysis (n = 45), and (2) therapeutics, intervention and management (n = 13). Most of the initial search results were filtered out as they focussed on co-morbidities such as rhinosinusitis or allergy in general. In addition, most of the other search results touching on rhinitis did not discuss children <6 years old separate from older children.
Additional information on the progression of rhinitis was obtained with the following key search terms: 'rhinitis' and 'natural history' (n = 3). Additionally the search terms 'rhinitis' and 'management guidelines' were included (n = 3).
Fig. 1 illustrates the workflow of the literature search in this review.
Definitions and classifications
Several large professional bodies, ARIA (World Health Organization), American Academy of Asthma Allergy and Clinical Immunology Task Force and British Society of Allergy and Clinical Immunology have published guidelines of the definitions, classification and management of rhinitis [2, 7, 8]. There is currently no management guidelines dedicated to children and this constitutes an unmet need for the clinical management of rhinitis in this age group.
The definition appears to be clear cut. Rhinitis has been defined as a disease of the nasal lining presenting with symptoms of nasal itch, sneezing, runny and/or blocked nose [6-8]. The classification of rhinitis differs slightly between guidelines. The ARIA guideline separates rhinitis into allergic and non-allergic, for which NAR is further classified by the triggering factors into including infectious, hormonal, occupational, and idiopathic (previously termed as vasomotor rhinitis). On the other hand, the British Society for Allergy and Clinical Immunology has classified infectious rhinitis as a separate category from NAR. This classification maybe more appropriate for rhinitis in early childhood where infectious causes may play a predominant role [2, 9]. Fig. 2 is an adaptation of the classification of rhinitis appropriate for childhood. It is both clinically and epidemiologically difficult to differentiate infectious rhinitis from AR in young children [2, 10]. In addition, NAR may also be present with AR, a syndrome termed mixed allergic rhinitis, which may account for 50%-70% of AR cases [11].
Sinusitis often co-exists with rhinitis and the term 'rhinosinusitis' has been coined to reflect this. Nasal polyps are rare in children. Clinical symptoms of discharge (mucopurulent), nasal obstruction, headache and facial pain, and ear pain and pressure are common symptoms of sinusitis [12]. Diagnostic confirmation requires endoscopic examination and CT scan of the sinuses [2]. Endoscopic examination is, however, difficult to perform in young children. Additionally CT scan examination does expose the child to considerable radiation [13]. Hence the diagnosis of sinusitis in children is quite challenging to the clinician and often has to depend on clinical symptoms. Additionally, most of these studies were not accompanied by allergy testing, hence the diagnosis of AR is tentative. It could well be that 'AR symptoms' in this age group may not be sufficiently sensitive for the diagnosis of AR.
Epidemiology of rhinitis in infancy and preschool age
Cross sectional studies
Most cross sectional population studies on rhinitis in early childhood have used the validated rhinitis questions from International Study of Allergy and Asthma in Childhood (ISAAC). However, the definitions of AR used in these studies were not entirely identical (Table 1). Some assessed the presence of symptoms indicating AR (sneezing, runny or blocked nose outside of cold or flu). On the other hand, other studies imposed stricter criteria of the requirement of diagnosis by physicians.
The prevalence of rhinitis in preschoolers 0-6 years old various considerably and this may be in part related to the definitions and age groups included in each study. The prevalence of rhinitis symptoms in preschool age groups ranged from 2.8% to 42.7% (Table 1). This wide variation in rhinitis prevalence is very similar to data in school aged children. The ISAAC studies which used the same validated questionnaire also showed a wide variation of rhinitis globally [14]. The studies from Singapore show that the prevalence of rhinitis in preschoolers is substantial with prevalence of 25.3% in the 4 to 6 year age group [15] and a cumulative prevalence of 42.7% in the 2 year age group [16]. These rates are in fact comparable with that reported in the phase III of the ISAAC with rhinitis rates reported at 25.5% for Singapore schoolchildren 6-7 years old [17]. These studies indicate that the prevalence of rhinitis young children may be considerable.
Birth cohort studies
Birth cohort studies provide us with the opportunity to understand the onset and development of rhinitis (Table 2). Besides parental atopy, these studies have provided with information on environmental risk factors for the development of AR such as having siblings [18], environmental tobacco smoke exposure [19,20], traffic pollution [20].
The Isle of Wight birth cohort study has shown that the prevalence of AR continues to increase into adolescence whilst NAR peaks in the preschool age group and then lags behind AR thereafter [6]. Interestingly, gender had a distinct role where NAR was more common in the female gender especially in adolescence. A study from the Paris cohort with follow up till 18 months has shown that the prevalence of AR-like symptoms were 9.1% in these age groups [10].
It therefore appears that rhinitis in young children has a heterogenous etiology. There is a tendency to label these symptoms as AR; however, validation with IgE sensitization, which is often not studied especially in cross sectional is necessary to make a definitive diagnosis.
Putative risk and protective factors
Intrinsic factors such as male gender, presence of atopy markers (serum IgE and eosinophil count), personal history of eczema or wheeze and allergen sensitization are known risk factors for the development of AR [18, 21-25]. A study by Marinho et al. [26]also showed a dose-response relationship between sensitization by means of specific IgE and skin prick test test results in the risk of rhinoconjunctivitis. Parental, especially maternal, history of allergic symptoms is also a consistently reported risk of AR [21, 23, 27, 28].
Various environmental factors were found to increase the risk of rhinitis in children <6 years old. Pollution factors such as environmental tobacco smoke (ETS) exposure, moulds, and traffic pollution seem to be an important risk of rhinitis. ETS exposure was reported to increase the risk of rhinitis [19, 20]. However, this increased risk was not consistently found [18, 29]. Traffic related pollutions were suggested to be an adjuvant for allergen sensitization [30], which may explain its reported association with increased risk of rhinitis [30, 31].
Exposure to moulds and dust endotoxins in the home may be risk modifiers for rhinitis. A study by Codispoti et al. [18] showed an interesting finding that there was a bimodal shaped relation between dust endotoxin level and the risk of rhinitis. In this study, moderate levels of entotoxin concentration increased the risk of rhinitis. However, there were protective effects against rhinitis at low and high levels of endotoxins instead [18]. Another study of the association between exposure to components of dust and moulds suggested a possible protective factor, though it is only observed in one of the two groups of subjects [32].
Dietary patterns may have protective effects. Several studies have found extended period of breastfeeding to be protective [18, 33]. However, this protective effect was not consistently observed [18, 21, 23, 28]. Though the age of introduction of solid foods in general did not affect the risk of rhinitis [34], early introduction of fish into diet of infants were shown to be correlated to reduced risk of AR [23, 28, 33]. Interestingly a study was done to assess the correlation between maternal vitamin D intake during pregnancy and AR outcome at 5 years old where maternal vitamin D intake from food protected against rhinitis [35].
The role of viral infections
Respiratory virus infections have been suggested to play a significant role in the inception and exacerbation of asthma [36]. The biological link between respiratory virus infection with wheezing and asthma had been also been studied widely [37]. Birth cohort studies focused on studying asthma have shown that respiratory viruses are commonly detected in infants and young children with rhinorrhoea [38, 39]. Till date, there have not been published data on the role of respiratory virus on the inception of AR or long-term rhinitis symptoms. Regardless, the same set of viruses suggested related to asthma, such as human rhinovirus, respiratory synctitial virus, human parainfluenza virus, human influenza virus and human coronavirus, have been detected in infants with upper respiratory tract infection and rhinorrhea [40]. Since respiratory viruses have been shown to cause inflammatory changes in the upper airway as has been seen in the lower airway [41], it is plausible for respiratory virus infections to play a role in the development of AR or NAR. An ongoing birth cohort study in Singapore (GUSTO; http://www.gusto.sg/) will focus on this role of early respiratory viruses infections in development of rhinitis including AR.
Burden and co-morbidities
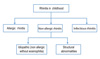
Besides its direct effect on the quality of life, rhinitis has significant co-morbid disorders (summarised in Fig. 3). The ARIA recommendations emphasizes the concept of treating upper and lower airway disorders as 'one airway, one disease' which includes a holistic approach towards the management of co-morbidities such as asthma, sinusitis, otitis media and conjunctivitis [42].
Adenoidal hypertrophy may be associated with AR [43]. Conversely adenoidal hypertrophy may mimic the symptoms of AR and therefore should always be considered in young children diagnosed with a diagnosis of AR [7]. Otitis media with effusion is often a co-morbidity of AR and NAR and should be evaluated in all young children with rhinitis. Recent onset otitis media with effusion in children [44] or occurring in the first 2 years of life [45] is associated with rhinitis at 6 years of age.
Management of rhinitis
The management of rhinitis and its co-morbidities in young children may require a multidisciplinary approach involving the paediatrician or paediatric allergist and the otolaryngologist. Fig. 4 is a suggested management strategy for young children with rhinitis.
A significant unmet need lies in the pharmacological armamentarum that is approved for use in children less than 2 years of age. First generation antihistamines are not recommended due to its sedative effect [2, 7, 8]. A second generation antihistamine, fexofenadine, had been tested to be safe in children 2 years old or older for management of AR [46] and from 6 months for chronic urticaria . Cetirizine and desloratidine have approval of use for AR in children as young as 6 months of age.
Intranasal corticosteroids such as mometasone furoate and mometasone diproprionate have age limit approval from 2 years and above (with the exception for EMEA for mometasone diproprionate where approval is for 6 years and above). Intranasal application of medications may also be challenging in terms of the child's co-operation with the application. In a recent study in Singaporean children about a quarter of children prescribed topical nasal medications refused to comply with therapy [47]. Montelukast is an additional anti-inflammatory agent that is approved for use for AR in children above the age of 6 months. However, a meta-analysis on very limited data in children, on comparative data between antihistamines, leukotriene receptor antagonists and intranasal corticosteroids showed that intranasal corticosteroids were the most effective for relief of AR [48].
Non pharmacological therapy with saline nasal rinses has also shown modest improvement in rhinitis symptoms in those above the age of 6 years [49].
Allergen immunotherapy is another therapeutic strategy that is attractive in that it reduces new sensitizations, reduces the risk of asthma and has a long term carry over effect even after cessation of therapy [2].
CONCLUSION
Rhinitis in young children is common with significant morbidity. There are significant gaps in our knowledge in terms of classification and phenotyping rhinitis in this age group. There are many unmet needs in the management and treatment guidelines are lacking. The WHO ARIA guidelines currently devote only 4 pages to childhood rhinitis in a document of 153 pages including references [2].





 XML Download
XML Download