

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anxiety control remains an important concern in dental practice, particularly with regard to minor oral surgeries. Although pain elimination techniques using local anesthesia have progressed, injection of the local anesthetic itself is so painful that the dental treatment is perceived as painful and invasive by most patients. Anxiety and dental fear continue to pose significant problems to both patients and dentists. Pain and anxiety control is fundamental to the practice of dentistry. Several previous studies have reported successful outcomes of moderate sedation for the treatment of dental anxiety in different types of patients undergoing a wide variety of dental procedures, without serious complications [12345]. Among all moderate sedation techniques, intravenous sedation is the most popular because of the rapid onset of action and ease of sedation level control [6]. Fentanyl and midazolam are commonly used in combination, although their mechanisms of action are different. While midazolam is a benzodiazepine with sedative and hypnotic qualities, the ability to cause powerful amnesia, and a short half-life, fentanyl is an opioid analgesic. However, moderate intravenous sedation is not without complications, with the reported incidence ranging from 0.5% to 25% depending on the type of medications used and their dosage, the type of patient, the procedure being performed, and the preferred level of sedation [7891011].
The purpose of this retrospective study was to evaluate the incidence, nature, and sequelae of complications during and after minor oral surgeries performed under intravenous midazolam and fentanyl sedation using the titration technique.
MATERIALS AND METHODS
Following approval from the Institutional Review Board of the Faculty of Dentistry and Pharmacy at Mahidol University (MU-IRB; COA No.MU-DT/PY-IRB 2016/017.1103), we retrospectively evaluated the medical records of patients who had undergone minor oral surgeries under moderate intravenous sedation with midazolam and fentanyl at our institution between January 1, 2015 and December 31, 2015.
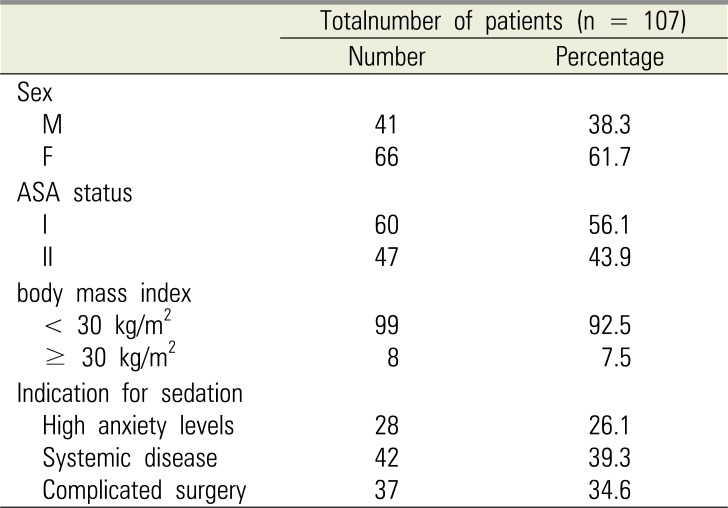
In total, 107 patients were enrolled, including 38.3% (41/107) men and 61.7% (66/107) women with a mean age of 43 years (range, 9–84 years). The patients were referred to the Anesthesia Unit for sedation by oral and maxillofacial surgeons if their anxiety levels were too high to be managed with local anesthesia alone, if they had systemic disease necessitating sedation, or if they required complicated surgery. Following preoperative evaluations by thorough history taking and physical examinations, patients were consulted as necessary. Preoperative vital signs, including blood pressure, heart rate, respiratory rate, and oxygen saturation, were recorded. All patients and/or their parents received written and verbal instructions, including explanations of the risks and benefits of the procedure, before surgery. They could not eat or drink for 8 h before their appointment, with the exception of medications, which could be consumed with a sip of water at least 2 h before surgery.
The minor oral surgical procedures included simple and complex tooth extractions, dental implant placement, sinus lift, miniplate removal, torus palatinus or mandibularis removal, and odontogenic cyst enucleation. Sedation was achieved by two anesthesiologists using the same protocol. To maintain an oxygen saturation of > 95% during surgery, a nasal cannula with 100% oxygen at 3 L/min was placed after the establishment of intravenous access. Midazolam and fentanyl were used for moderate intravenous sedation. First, fentanyl 0.5 to 1 mcg/kg was administered according to the patient's age and presence of comorbidities. Then, midazolam was titrated at 0.5 to 1 mg/min until a Ramsay score of 3–4 was observed [12]. A 2% solution of mepivacaine with 1:100,000 adrenaline was infiltrated in all patients, and the procedure was initiated once the surgical area was completely anesthetized. During the surgery, additional doses of fentanyl and midazolam were administered as necessary to maintain a Ramsay score of 3–4. Vital signs, including blood pressure, respiratory rate, heart rate, and oxygen saturation, and electrocardiograms were recorded at 5-min intervals. If the oxygen saturation reached 95%, the anesthesiologist would promptly stimulate the patient to take a deep breath. After the completion of surgery, consciousness levels and vital signs, including blood pressure, heart rate, and oxygen saturation, were monitored until they met the hospital discharge criteria (Aldrete score ≥ 9). Then, patients were allowed to leave with their escort, with written information regarding postoperative care pertaining to the surgery and anesthesia.
Age, sex, body mass index, medical history, American Society of Anesthesiologists (ASA) classification, indications for sedation, amount of sedative used, surgical duration, recovery time (time from completion of surgery to the time when the patients met the discharge criteria), sedation-related complications, and failures were evaluated for all patients.
All data were coded for computer analysis using the Statistic Package for Social Sciences (SPSS version 13). Continuous variables are expressed as means and standard deviations and categorical variables are expressed as numbers (percentages). The significance of differences between patients with and without sedation-associated complications was assessed using t-tests for continuous data and χ2 tests and Fisher's exact tests for categorical data. A P-value of < 0.05 was considered statistically significant.
RESULTS
In total, 107 patients were enrolled, including 60 (56.1%) with ASA class I and 47 (43.9%) with ASA class II. The most common systemic disorders were hypertension (31/107). The mean body mass index (BMI) was 22.8 ± 4.4 kg/m2, and eight (7.5%) patients with a BMI of ≥ 30 kg/m2 were considered obese. Of the total, 26.1%, 38.3%, and 34.6% patients were sedated because of high anxiety levels, systemic disease, and complicated surgical procedures, respectively (Table 1).
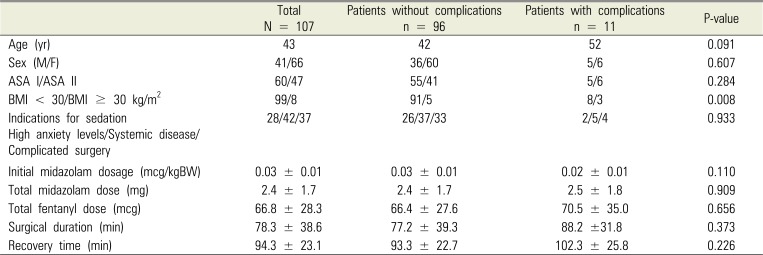
The mean initial midazolam dose required to achieve a Ramsay score of 3–4 was 0.03 ± 0.01 mcg/kg, the mean total midazolam dose was 2.4 ± 1.7 mg, the mean total fentanyl dose was 66.8 ± 26.3 mcg, the mean surgical duration was 78.3 ± 38.6 min (range, 14–205 min), the mean recovery time was 94.2 ± 23.1 min (range, 60–150 min), and the incidence of sedation-related complications was 10.2% (11/107; Table 2). During surgery, the oxygen saturation reached 95% after administration of the initial doses of midazolam and fentanyl in six patients, who were successfully managed by stimulation to take a deep breath. Two patients experienced difficulty in following commands after administration of the initial doses and were considered to be under deep sedation, while one patient exhibited paradoxical excitement. After surgery, one patient experienced nausea without vomiting and one exhibited a prolonged recovery time (time from completion of surgery to time of meeting the discharge criteria, > 120 min). The surgical procedure was completed in all patients. Table 2 shows differences between patients with sedation-related complications and those without complications with regard to age, sex, ASA classification, BMI, indications for sedation, initial midazolam dosage in mcg/kg, total midazolam and fentanyl doses, surgical duration, and recovery time. The mean age, total midazolam and fentanyl doses, surgical duration, and recovery time were greater for patients with complications than for those without complications. However, none of the parameters showed significant differences between the two groups. The incidence of sedation-related complications was significantly higher for obese patients than for nonobese patients (P < 0.05).
DISCUSSION
Sedation is a major part of many dental procedures, particularly minor surgical procedures, which are always invasive and cause pain and discomfort. Oral surgery is ranked high on anxiety rating scales by patients, and sedation is recommended for anxiolysis [13]. Most patients requiring oral surgery can be managed with a local anesthetic alone. However, there are instances where moderate sedation can make otherwise uncomfortable treatment experiences acceptable. Certain medical conditions requiring stress reduction protocols can be managed more safely by using sedation as an adjunct to local anesthesia. It is well documented that sedation is a continuum and not a static point that can be achieved with a specific drug or dose, and it can vary from patient to patient or even within an individual patient.
However, the practice of moderate sedation is not free of risks. Fortunately, serious complications such as permanent neurological deficit or death are rare after the implementation of standards of care, including training, monitoring, and quality assurance [1415161718]. Sedation-related complications include respiratory depression caused by oxygen desaturation or apnea, hemodynamic fluctuations, nausea and vomiting, and paradoxical excitement.
The intravenous moderate sedation procedures in the present study involved the use of fentanyl and midazolam for sedation and pain control. The rate of sedation-related complications was 10.2%. Wilson et al. [7] reported a complication rate of 3% in anxious dental patients sedated with intravenous midazolam, while Rodgers et al. [8] reported a rate of 1.57% for patients who underwent oral surgery under intravenous sedation. Furthermore, Inverso et al. [9] reported a complication rate of 0.5% for patients who underwent third molar extraction surgery under moderate sedation, Sanel et al. [10] reported a rate of 1.4% for patients who underwent oral and maxillofacial surgery under intravenous sedation with midazolam and fentanyl, and Kouchaji [11] reported a postoperative complication rate of 25% in individuals with intellectual disability who underwent dental treatment under intravenous sedation with propofol. The sedation-related complication rate observed in our study was somewhat higher than these previous rates. However, it is difficult to compare our study with the other studies. The disparity in results between our study and the previous studies is partly due to differences in the definition and recording of adverse events. For example, the definitions of oxygen desaturation vary from 80% to 95% over periods of time that span a single instant to a requisite duration of up to 60 s.
Currently, there are no established definitions or terminologies for sedation-related adverse events. The International Sedation Task Force (ISTF) of the World Society of Intravenous Anaesthesia (World SIVA) has defined an oxygen saturation of 75–90% for < 60 s as a minor risk descriptor and an oxygen saturation of < 75% for any time period or < 90% for > 60 s as a sentinel risk descriptor [19]. In our study, patients were promptly stimulated to take a deep breath when their oxygen saturation reached 95%. Because of this quick intervention, neither apnea nor desaturation was observed. Although a decrease in oxygen saturation may be brief or may resolve spontaneously, we considered this situation as a complication in our study. All other complications were minor. Two patients experienced deep sedation, although the oxygen saturation was maintained at > 95%, and one patient exhibited paradoxical excitement, represented by increased talking. One more patient experienced nausea without vomiting after surgery, which resolved by adequate rest without any intervention. Finally, the planned procedures were completed in all patients.
We could not find a relationship between the occurrence of sedation-related complications and age, sex, ASA classification, indications for sedation, initial midazolam dosage per kilogram body weight, total midazolam dose, total fentanyl dose, surgical duration, and recovery time.
However, the incidence of sedation-related complications was higher in obese patients than in nonobese patients (P < 0.05). All three obese patients who experienced sedation-related complications exhibited an oxygen saturation of 95% after administration of the initial midazolam and fentanyl doses. Inverso found a 72% increase in the adverse event rate with an increase in the ASA class to the next level, whereas Sanel did not find a relation between the medical status and complication rate, similar to the finding in our study. However, our study was limited by the small sample size, and further studies with larger samples including different types of patients and procedures will strength our results and enable the clinical application of our findings with greater confidence. No serious complication was observed in the present study, similar to findings in previous studies [7891011].
In conclusion, our results suggest that complications associated with moderate intravenous sedation with midazolam and fentanyl using the titration technique are minor and can be successfully managed within the dental department, with no prolonged sequelae. Compared with general anesthesia, this method required less resources and is useful for the management of patients undergoing oral surgery.
 XML Download
XML Download