

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Third molar surgery is one of the most common procedures performed among all oral and maxillofacial surgeries [1]. Most surgical procedures of the lower impacted third molar (LITM) are usually performed under local anaesthetic; it requires a highly effective local anesthetic to achieve a sufficient nerve block [234].
An inferior alveolar nerve block (IANB) [5] is the most frequently used injection for LITM surgery. However, it has been previously reported by multiple studies that IANB does not always successfully achieve pulpal anesthesia for the entire duration of the operation and has a reported failure rate of 17% to 58% [6789]. Apart from a failed IANB, many intra-operative and post-operative complications, such as pain and limited mouth opening, needle breakage at that point of injection, and hematoma, have been reported [123].
In recent years, there have been several studies regarding the infiltration at the lower first molar, which is done for several reasons, including anesthesia for pulpal treatment and as an anesthetic supplement for LITM without using IANB [4567]. The study by El-Kholey [8] shows that infiltration at the buccal vestibule of the mandibular first molar with 3.6 ml of 4% articaine with supplemental lingual anesthesia may be a good option for LITM removal. In addition, the study by Lima-Júnior et al. [9] found that most mandibular extractions could only be performed with mandibular vestibule anesthesia. However, Zain et al. [6] found that mandibular buccal infiltration can be considered an available alternative to IANB in securing successful pulpal anesthesia for endodontic treatment. Similarly, the study by Kanaa et al. [10] found that articaine infiltration produced significantly more episodes of no response to maximum stimulation in lower first molars than did lidocaine. Therefore, Zain et al. [6] concluded that buccal infiltration with 4% articaine in the mandible can be considered available alternative to 2% lidocaine IANB for ensuring successful mandibular pulpal anesthesia for endodontic therapy.
Fowler et al. evaluated the success rates for the inferior alveolar nerve block and buccal infiltration of 4% articaine in the molar and premolar regions [11]. While Abazarpoor et al. [12] also studied the success rate of IANB when the volume of 4% articaine is increased in mandibular anesthesia.
There are no studies regarding 4% articaine infiltration injection in the retro-molar area for LITM surgery. Therefore, the purpose of this study was to compare the efficacy of double cartridges of 4% articaine for infiltration at the retro-molar region of the mandible and the onset of anesthesia with a single cartridge of 4% articaine, profoundness of analgesia, and duration of anesthesia in LITM surgery.
MATERIALS AND METHODS
1. Patients and methods
This study was approved by Committee in the Ethics of Research in Human Being of Dentistry and Pharmacy Mahidol University Institutional Review Board with Protocol No. MU-DT/PY-IRB 2016/DT032. The procedure was explained to all patients and written consent was obtained from each patient prior to the operation.
The patient selection in this study consisted of 30 patients, which was calculated according to power. The sample consisted of 9 men (30%) and 21 women (70%), with a mean age of 20 years (range = 18 to 25 years).
The patients had symmetrical LITM as seen on panoramic radiographs. The patients underwent 2 surgical interventions by 2 expert surgeons, one for the local anesthetic injection and another for LITM surgery. An expert dentist determined the measurement parameters with a 3- to 4-week washout period. Before injection of the local anesthetic, all patients had their pain perception and pulpal sensitivity measured on a healthy canine and first or second molar that were ipsilateral to the third molar scheduled for removal.
2. The eligibility criteria
The inclusion criteria were patients who were aged between 18 and 30 years, healthy, non-smoker, and non-alcoholic, had LITMs that were symmetrically positioned on both sides of the mandible, at least one healthy lower first or second molar on both sides without caries or restoration, and the ability to provide their consent for the study and understand and carry out the instructions given by the investigators.
Patients with systemic diseases including hypertension, cardiovascular problems, renal and/or liver failure or other serious medical condition, who were pregnant or currently lactating, allergic to local anesthetics, had facial deformities that would interfere with the injections for surgery or evaluation were excluded from the study. In addition, patients who presented with swelling and/or infection associated with the LITM site, taking any kind of medication during the 5 days prior to surgery that would alter their perception of pain (analgesic, antidepressants,), and patients who were not able to follow instructions or cooperate during the study were excluded. A patient was free to withdraw their participation from the study at any time based on their own decision.
Before the operation, a preoperative measurement with an electrical pulp test (EPT) at the canine and molar was recorded as “EPT pre-operative.” In addition, blood pressure was also recorded at baseline. The patients were assigned to receive a local anesthetic with either double cartridges (DC), which consisted of 3.4 ml of 4% articaine with 1: 100,000 epinephrine or single cartridge (SC), which consisted of 1.7 ml of 4% articaine with 1: 100,000 epinephrine during each operation. Infiltration was administered in the retro-molar mucosa region without anesthesia of the lingual mucosa as shown in Fig. 1. After 10 minutes of the injection, EPT was evaluated and recorded to confirm of pulpal anesthesia. Subsequently, removal of the LITM was initiated following standard surgical techniques.
During the operation, blood pressure and pain score were recorded at every step. The amount of additional local anesthetic administered, total volume of anesthetic injected, onset of anesthesia, and the operation time were recorded.
Postoperatively, all patients were instructed to complete a Patient Record Form in order to evaluate the duration of anesthesia, as indicated by the recovery of sensation on the lower lip, and recorded any unfavorable events that occurred postoperatively. Postoperative medications were oral paracetamol 500 mg administered every 4 to 6 h for pain and oral amoxicillin 500 mg administered 4 times a day for 5 days.
3. Statistical analysis
The differences in the variables used to measure the outcome between 2 studies in the same patient were compared using a paired t-test or Wilcoxon's signed rank test. The following were the outcomes of interest: the visual analog scale (VAS) while local anesthetic was being disposed and immediate post-operative pain, the scoring of the intra-operative numerical rating scale, delete it, objective onset, distribution of the patients according to the occurrence of pulpal sensibility at baseline and after 10 minutes, operation time, duration of anesthesia, and intra-operation intensity of pain. McNemar's test was used to calculate the distribution of the cases according to the success and failure of the analysis of the 2 groups. Pearson correlation, Chi-square, and Mann-Whitney U tests were used to evaluate the correlation of variables with the success rate.
RESULTS
The success rate of the DC versus SC of 4% articaine was statistically significant with a P-value < 0.05. The total volume of anesthetic in the SC and DC groups were also significantly different (P-value < 0.05) as shown in Table 1.
The type of impaction and difficulty were accessed using a panoramic radiograph. All of the impactions were symmetrical. Fig. 2 shows the angulation and position of LITM surgery in this study.
Table 2 shows the onset of local anesthesia and there was no significant difference (P > 0.05) between the groups despite the fact that the DC group had early onset of anesthesia compared to the SC group. The duration of anesthesia in DC group was statistically superior to SC group (P < 0.05). However, the difference in surgical time between SC and DC had no statistical significance (P > 0.05).
A prolonged EPT response was defined by the difference between the EPT value pre-injection and 10 min post-injection, as shown in Fig. 3. The DC group had a significantly more prolonged EPT response (P < 0.05) at the canine and molar than the SC group. Table 3 shows that a more prolonged EPT response in the molar area is correlated with a higher success rate of anesthesia in both groups with high statistical significance in both the groups (P < 0.05).
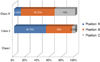
The SC group required a Position A supplemental anesthesia injection during the osteotomy and tooth removal steps, whereas the DC group required additional anesthesia during the odontectomy and tooth removal step (Fig. 4).
Fig. 5 shows that the pain intensity gradually increased during the operation and peaked at the tooth removal step, after which it nearly returned to baseline in the finishing suture step. However, there seem to be differences between the data from both groups at each step, but significant difference (P > 0.05) was not observed in terms of the general pain intensity. However, the VAS of post-operative pain was significantly higher in the SC group than in the DC group (P < 0.05).
DISCUSSION
It has been mentioned by Professor Malamed [13] that unlike other amide local anesthetic drugs that contain a benzene ring, articaine contains a thiophene ring, which increases its lipid solubility. Lipid solubility determines the degree of penetration of the molecules into nerve membranes. Therefore, articaine diffuses better through soft tissues than do other anesthetics, thereby achieving higher intra-neural concentrations, more extensive longitudinal spreading, and a better blockade of conduction. A second molecular difference between articaine and other amide local anesthetics is the extra ester linkage incorporated into the articaine molecule, which results in hydrolysis of articaine by plasma esterase.
Local infiltrate technique with 4% articaine was an effective method of anesthetizing a mandibular tooth [1014]. The study by Fowler et al. mentioned the success rates for the inferior alveolar nerve block and buccal infiltration of 4% articaine of the molars and premolars would not be different for pulpal anesthesia [11]. Articaine is commonly used in the dental and medical fields. Topical or local infiltration administration of articaine proved to be sufficient for dental procedures requiring anesthesia with a short to intermediate duration of action and a fast onset[15]. Senes et al. found that 2% articaine and 4% articaine with 1:100,000 epinephrine that were administered in equal volumes were equally effective and safe during LITM surgery [16]. Abazarpoor et al. [12] reported that increasing the volume of 4% articaine provided significantly more successful IANBs in mandibular anesthesia and did not result in 100% anesthetic success.
This study was conducted to evaluate the efficacy of different volumes of 4% articaine as infiltration anesthetic at the retro-molar region for surgical LITM removal. Group 1 received a SC of 4% articaine and group 2 received a DC of 4% articaine with the same concentration of 1:100,000 epinephrine. The results suggested that infiltration with a DC of articaine had better clinical efficacy than a SC of articaine in LITM surgery without any adverse clinical effects. The duration of anesthetic effect, amount of additional anesthetic administered, total volume of anesthetic used, success rate of local anesthetic, and profoundness of pulpal anesthesia were significantly different between the two doses of articaine used. However, the duration of surgery was not significantly different between the groups.
The DC of 4% articaine had faster onset of action than did the SC of 4% articaine, but this was not significantly different. A previous study suggested that the onset of local anesthesia is unaffected by the volume of local anesthesia used [17]. However, it has been mentioned that the onset of local anesthesia was influenced by the pH of the solutions and the pH of physiological tissue [1318].
The duration of anesthesia for a DC of 4% articaine in this study had soft tissue anesthesia for approximately 292.9 ± 79.66 minutes. This is consistent with the results of a previous study in which soft tissue anesthesia with 2% lidocaine and 1:100,000 epinephrine ranged from 240 to 300 min [192021]. On the other hand, the duration of anesthesia for a DC of 4% articaine was statistically superior to that of a SC of 4% articaine. The higher volume of local anesthesia might be related to the duration of soft tissue anesthesia [21]. Hence, a DC of 4% articaine had a longer duration of anesthetic action than a SC of 4% articaine.
EPT is used to indicate the level of profoundness of pulpal anesthesia after administration of a local anesthetic in endodontic treatment [17]. In this study, there was difference in the EPT response for the examined teeth 10 min post-injection between the groups; the DC of 4% articaine group had higher EPT response than the SC group with statistical significance. In addition, the EPT response was significantly correlated with the success rate in both groups. These results are consistent with results from previous studies that suggest greater volumes of anesthetic solutions are more efficacious for pulpal anesthesia [12].
In this study, 5 cases that received a DC of 4% articaine required additional anesthesia, although subjective symptoms, such as numbness of half of the tongue and lower lip on the injection side, were suggestive of complete anesthesia. Perhaps, the failure to appropriately inject or the lack of effectiveness of a SC to produce objective symptoms completely might be attributed to the requirement of additional doses of anesthesia. Moreover, additional local anesthetic in the SC group was needed more frequently during the operation. This requirement was significantly higher during the tooth removal stage. This contradicts the results of previous studies in which insufficient pain control requiring additional anesthetic occurred during the odontectomy stage [8].
The pH of the local anesthetic solution has been recognized to likely produce a burning sensation in the tissue during administration [13]. In this study, 4% articaine was used in both groups. However, the incidence of pain while the drug was being injected was not significantly different in our study despite the differences in volume of the drug delivered. These results also contradict those from previous studies that found a higher volume of anesthesia created more pain during an injection due to the pressure from a greater volume of anesthetic [22].
In conclusion the double cartridges of 4% articaine with 1:100,000 epinephrine provides a more effective infiltration when compared to a single cartridge of 4% articaine with 1:100,000 epinephrine for surgical removal of LITM with a higher success rate, longer duration of anesthesia, less intra-operative pain, and less additional anesthesia. The higher volume of 4% articaine can be considered for use as infiltration since it has no adverse reactions in healthy adult patients.







 XML Download
XML Download