

 PDF
PDF ePub
ePub Citation
Citation Print
Print


DEFINITION
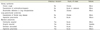
Aspiration simply means to draw in or out by means of suction. In patient care, the term aspiration is often used to describe the inflow of material from the oral cavity or upper gastrointestinal tract into the lungs through the larynx. The term itself does not reflect the nature of the material or the specific outcome of the event [1]. The material that can be aspirated varies and includes saliva, nasopharyngeal secretions, bacteria, liquids, toxic substances, food, or gastric contents. The outcome of the event also varies widely; it can remain within the spectrum of normal physiology or result in very severe conditions such as acute respiratory distress syndrome (ARDS) [23]. Most the clinical outcomes are outlined in Table 1. These manifestations of aspiration are categorized based on three key characteristics, including the infectiousness of the inoculum, volume of the inoculum, and acuity of the onset of the clinical syndrome [4]. Important manifestations that induce sudden changes in the patients' conditions and are troublesome for the clinicians, especially for the intensive care unit (ICU) health providers, are aspiration pneumonitis (chemical pneumonitis) and aspiration pneumonia (infectious process secondary to an aspiration event) caused by macroaspiration. However, aspiration can be silent (unwitnessed), and it is difficult to distinguish between these two manifestations [25].
Aspiration pneumonitis is defined as a condition that shows immediate hypoxemia, fever, tachycardia, and abnormalities on chest radiograph, which is caused by macroaspiration of noxious liquids. The noxious fluids are mostly sterile gastric contents; although they can be also bile or other agents introduced through the stomach [4]. In an animal model, the pathophysiology of chemical pneumonitis has been suggested to be distinguishable from subclinical aspiration based on the pH and volume of the gastric material. To induce severe inflammation in the experiment using human gastric secretions and rabbit lungs, a pH below 2.4 was required [6]. In a dog model with induced chemical pneumonitis, more than 2 ml of hydrochloric acid solution per kilogram were required to induce a clinical syndrome [78].
Aspiration pneumonia generally implies acute lung infection that occurs after aspiration of oropharyngeal or upper gastrointestinal contents in large volumes. The aspirated contents are often not acidic enough (likely a pH much greater than 2.5) to induce chemical pneumonitis. Bacterial load introduced from the oral cavity or upper gastrointestinal tract is normally nonvirulent and are usually anaerobic organisms, capable of inducing lung infections due to their large volume [69]. However, despite attempts for a more clear-cut classification, there is still confusion surrounding the terminology and the precise definition [10].
INCIDENCE AND EPIDEMIOLOGY
Gastric aspiration is a known complication of general anesthesia with an incidence of one in every 2,000–30,000 cases [1112]. Moreover, it has been recently estimated that aspiration occurs roughly in 3 every 10,000 anesthetic procedures, with higher frequency in special populations and emergency situations [13]. Dental treatment for disabled or handicapped patients often requires general anesthesia or sedation due to the patients' inability to cooperate with the procedure. These patients often have general medical issues along with dental problems such as poor oral hygiene, and consequently a higher chance of anesthetic complications, particularly aspiration-related [1415]. One study reported aspiration pneumonia in 12 (9.8%) out of 123 elderly patients (> 65 y old) who survived cardiovascular surgery and final extubation [16]. Moreover, aspiration frequently occurs in ICU patients, elderly, and nursing home residents [1718]. A case-control study on nursing home-acquired pneumonia patients and community-acquired pneumonia patients has reported an incidence rate of 18% and 5%, respectively [19].
However, most cases of aspiration events are either silent or unwitnessed; accordingly, the true incidence rate of aspiration-induced lung injury is difficult to estimate. A prospective study that used the bronchoalveolar lavage level of pepsin as a surrogate marker of aspiration in ICU patients has reported that 88.9% of the patients had at least one aspiration event [20]. Unwitnessed gastric aspiration is thought to be important to explain many cases of perioperative pulmonary dysfunction. However, most aspiration pneumonitis cases are often misdiagnosed as bacterial pneumonia, whereby the patients are consequently given the inappropriate treatment [518].
The severity of the lung injury after aspiration differs based on the content, amount, and acidity of the aspirate, as well as certain characteristics of the patients (i.e. oropharyngeal colonization or host defense mechanisms); it also varies widely from mild and subclinical pneumonitis to progressive respiratory failure. In a retrospective study on patients who underwent general anesthesia, Warner et al. [12] have reported a total of 66 patients who had aspiration, out of which 42 were asymptomatic, 13 required mechanical ventilation for more than 6 hours, and 3 patients died. Gastric aspiration is a direct key cause of severe ARDS [2122]. More severe and persistent ARDS occurs in about 1/3 of the aspiration pneumonitis patients [2324]. The incidence of ARDS in the United States varies between 50,000–150,000 cases per year [2125 2627282930].
PATHOPHYSIOLOGY
Aspiration pneumonitis and aspiration pneumonia are clinically difficult to distinguish. Although there is some degree of overlap, the two aspiration syndromes are separate disease entities with distinguishable pathophysiology.
First, aspiration pneumonitis is an acute lung injury caused by macroaspiration of refluxed gastric contents. Since 1946, when Mendelson described aspiration pneumonitis as the Mendelson's syndrome, the importance of acid has been emphasized [31]. Mendelson demonstrated that severe pneumonitis induced by acidic gastric contents in the rabbit's lung was comparable to the same condition induced by the same amount of 0.1 N hydrochloric acid. Subsequently, a study using adult rats has shown that the aspiration of diluted hydrochloric acid (pH 1.25) resulted in a characteristic biphasic response against lung injury [32]. The first phase was a direct, corrosive effect of low pH on the airway's epithelium, with a peak timing of 1–2 hours after acid aspiration. The second phase was a neutrophilic inflammatory response, which occurred 4–6 hours after aspiration. The mechanism of lung injury after acid aspiration involves inflammatory mediators, inflammatory cells, adhesion molecules, tumor necrosis factor α, interleukin-8, enzymes (cyclooxygenase, lipooxygenase), and reactive oxygen species. Among these factors, neutrophils and complement play pivotal roles [33343536373839].
Gastric contents include not only acid but also food particles. Animal experiments on lung injury by gastric food particles have used small non-acidified gastric particles (SNAP) obtained by washing, filtration, autoclaving, and centrifugation of the stomach contents from rodents [404142]. Acute neutrophilic inflammation was observed 4–6 hours after tracheal instillation of SNAP. However, in contrast to the acid model, a direct injury in the early stages was not observed [40].
The combined acid and small non-acidified gastric food particles, known as the CASP model (acid + SNAP), closely resembles the actual gastric aspiration. Lung injury due to CASP aspiration was more severe compared with lung injuries due to acid or SNAP alone, in both rats and mice [434445]. In the CASP model, the bronchoalveolar lavage level of albumin—an index for loss of alveolar-capillary integrity—was significantly increased compared with the acid or SNAP models. Moreover, the ratio of the arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FIO2) ratio, which reflects arterial oxygenation, was significantly lower compared with the other two models [41].
Gastric contents are sterile under normal conditions. However, changes in gastric pH to inhibit bacterial growth through use of antacids, H2-receptor antagonists, or proton-pump inhibitors can result in an environment where potentially pathogenic organisms become viable [4647]. Furthermore, gastric colonization due to gram-negative bacteria can occur in patients under enteral feeding or patients with gastroparesis or small-bowel obstruction [474849]. If gastric aspiration occurs under these conditions, lung infection from bacterial load in gastric contents can occur in addition to the acute inflammation due to acid or food particles; this is the case explaining overlap with aspiration pneumonia.
Aspiration pneumonia often occurs after aspiration of colonized oropharyngeal material. It can also occur when gastric aspiration occurs subsequently to gastric colonization. If the bacterial burden included in the oropharyngeal secretion is small, and the host defense mechanisms such as coughing, active ciliary clearance, and humoral and cellular immune system are intact, aspiration may not result in lung infection. However, if mechanical, humoral, and cellular defense mechanisms are impaired and the volume of aspirate is sufficiently abundant, aspiration pneumonia can occur [5]. Factors that increase the risk of oropharyngeal colonization of potentially pathogenic organisms and growth of bacterial load in consequently increase the risk of aspiration pneumonia. Indeed, the risk of aspiration pneumonia is low in patients without teeth [50] and in patients under aggressive oral care [51].
Bacteriology is important in explaining the unique pathogenesis of aspiration pneumonia. Compared to previous studies that suggested the anaerobic bacteria as the key pathogen of aspiration-induced lung infection [525354], recent studies have demonstrated a reduced role of anaerobes not only in aspiration pneumonia but also in lung abscess or empyema [5556575859]. The discrepancies may be due to the difference in timing and method of obtaining the microbiologic specimens, as well as the patient characteristics. Etiologic bacteria for aspiration pneumonia are now categorized as community-acquired or hospital-acquired, and are similar to community-acquired pneumonia or hospital-acquired pneumonia [60]. This result may be reflecting the changes in the pathogenesis. In the past, only bulky aspiration of anaerobic normal flora was a key mechanism, but recent studies suggest that oropharyngeal colonization of pathogenic organisms prior to the aspiration event is thought to be an important step in addition to large-volume aspiration.
RISK FACTORS
Aspiration is frequently observed in patients with conditions including altered mental status, dysphagia or swallowing dysfunction, esophageal motility disorders, gastrointestinal disorders, and enteral tube feeding. Predisposing conditions of aspiration-induced lung injury are undoubtedly related to risk factors such as frequent and/or large-volume aspiration and oropharyngeal or gastric colonization that provide the infection source. However, it is difficult to derive a comprehensive conclusion on independent factors that are directly linked to aspiration pneumonitis or aspiration pneumonia. This is due to multiple reasons including the inconsistent use of terms related to aspiration, i.e., aspiration pneumonitis and aspiration pneumonia among different studies, patient demographics that can act as an uncontrollable confounding factor, and presence of comorbidity [6162]. However, special care for the patients with risk factors of aspiration is undoubtedly needed to prevent aspiration-induced lung injury.
Adnet and Baud [63] have reported that the risk of aspiration increases with the degree of unconsciousness measured using Glasgow coma scale. Aspiration pneumonitis is associated with acute unconsciousness from sedation, poisoning, or trauma [3164]. Vomiting and large-volume reflux of gastric contents, which frequently occur in unconscious patients, are likely to increase the risk of aspiration pneumonia.
Dysphagia is a complication associated with neurologic diseases such as dementia, Parkinson's disease, multiple sclerosis, and stroke. Dysphagia increases the aspiration risk of oropharyngeal contents and is associated more closely with aspiration pneumonia than with chemical pneumonitis based on the pathophysiology [965]. The swallowing mechanism is also affected by the anatomy of the chest. Swallowing dysfunction is frequently observed in patients with a hyperinflated chest anatomy due to the chronic obstructive pulmonary disease (COPD). Previously, patients with COPD displayed defects in the laryngeal elevation during swallowing compared with controls, necessitating the use of protective swallowing strategies [66]. It has been recently reported in nursing home residents and post-stroke populations that COPD is a risk factor for aspiration pneumonia [6267]. Other common risk factors of frequent or large-volume aspiration are outlined in Table 2.
In addition to the aspiration risk factors, microbiologic factors affect the occurrence risk of aspiration pneumonia, which increases depending on the number of microbes in the oropharyngeal or gastric aspirate and virulence. Previous studies have suggested that factors related to oral hygiene are associated with the occurrence of pneumonia [6869]. Dental or gingival diseases increase the oral microbial density and virulence. Consequently, the occurrence risk of pneumonia increases when aspiration occurs. Terpenning et al. [68] have analyzed the dental and oral risk factors associated with aspiration pneumonia incidence along with other medical risk factors. They identified the dental decay, presence of cariogenic bacteria, and periodontal pathogens as significant risk factors. One study observed oral cavities of elderly patients requiring long term care who contract aspiration pneumonia and described characteristic change like mucous membranes residues like oblate, coated tongue, or remaining roots after losing the crown portion. These factors were also suggested as environmental factors that induce colonization of bacterial flora, which are not observed under healthy oral conditions [70]. Proton pump inhibitors and histamine receptor-2 antagonists change the acidic gastric environment and promote gastric colonization. Although these drugs do not increase the risk of gastric aspiration, they are strongly association with pneumonia [7172].
DIAGNOSIS
Patients with risk factors for aspiration can be suspected of having aspiration in case they show acute symptoms such as coughing, choking, shortness of breath, cyanosis, tachypnea, tachycardia, speaking difficulty, and hoarseness [2]. Witnessed aspiration is evident by validating the presence of oral contents, food particles, pepsin, or bile in the trachea-bronchial tree or bronchoalveolar lavage fluid. In patients with severe trauma, blood-containing aspirates can be observed [73]. Following aspiration, if patients show acute inflammatory signs, such as fever, tachycardia, tachypnea, and leukocytosis, or respiratory symptoms/signs, such as cough, sputum, and hypoxia, combined with new or worsened infiltrates that can be observed on a chest radiograph, they may be suffering from an aspiration-induced lung injury. Moreover, patients are diagnosed with either aspiration pneumonia or aspiration pneumonitis with subsequent bacterial infection in case of a bacteriologic evidence of an infection. Patients with aspiration pneumonitis or pneumonia may progress to acute lung injury and acute respiratory distress symptom (ALI/ARDS), which is characterized by hypoxemia and respiratory failure. Thus, the work of breathing increases and lung compliance decreases, leading to pulmonary hypertension or cor pulmonale [2].
However, one of the reasons for difficult diagnosis is unwitnessed aspiration or silent (asymptomatic) aspiration. If lung injury is suspected without clear evidence of prior aspiration, the clinician is required to make a diagnosis by exclusion. Patients can be diagnosed with aspiration-induced lung injury if they exhibit risk factors for aspiration only after excluding other possible causes of hypoxia, such as pulmonary edema, pulmonary embolism, and community- or hospital-acquired pneumonia. Such diagnosis is possible if patients show radiographic evidence of infiltrate in dependent bronchopulmonary segment [574]. When the patient is in a recumbent position, the dependent pulmonary segments are the posterior segments of the upper lobes and apical segments of the lower lobes. During walking or in a semi-recumbent position, the basal segments of lower lobes are mainly involved [575].
Another challenge is to distinguish between aspiration pneumonitis and aspiration pneumonia. Clinical features assist in differentiating these two entities. Unlike aspiration pneumonitis, the aspiration event is not frequently witnessed in aspiration pneumonia [575]. If aspiration as a preceding event is not obvious, the patient is more likely to have aspiration pneumonia. A large volume of stomach contents is needed to induce chemical pneumonitis, resulting in a more evident aspiration events in cases of aspiration pneumonitis. Furthermore, the clinical course of aspiration pneumonitis is more rapidly progressing; hyper-acute hypoxemia occurs, and devastating lung injury can occur and be resolved within 48 hours. These patients are likely to exhibit symptoms such as bronchospasm, frothy sputum, and bilateral patchy infiltrates, even in nondependent lung fields [575]. Features that differ between aspiration pneumonitis and aspiration pneumonia are outlined in Table 3.
However, there is no gold standard to differentiate between these two entities. Due to these difficulties, there have been attempts to use biomarkers. El-Solh et al. [76] have reported the use of serum procalcitonin levels to distinguish between aspiration pneumonia and aspiration pneumonitis. Indeed, the serum concentration of procalcitonin increases under various bacterial and viral infections [77]. However, no significant differences in procalcitonin levels were observed between the negative-culture-group and the positive-culture-group of bronchoalveolar lavage fluid.
TREATMENT
The main principle of treatment is that immediate cares based on the symptomatology and progression of the disease is essential prior to any efforts to differentiate between aspiration pneumonitis and pneumonia. However, the direction of the treatment is different for the two conditions and consists of supportive management itself for aspiration pneumonitis and antimicrobial therapy for aspiration pneumonia [74].
If aspiration is witnessed or suspected, the patient's position should be adjusted to minimize the risk of additional aspiration. For conscious patients, the head should be rotated laterally, and suction is applied to the oral and pharyngeal cavities [78]. Humidified oxygen should be administered and nebulized bronchodilator is used if necessary. Furthermore, the head of bed is raised by 45 degrees. Indications for intubation are similar to the general indications based on the general neurologic status, degree of hypoxia, and hemodynamic stability. To facilitate bronchoscopy in large volume solid aspiration, intubation is preferred [7879]. Mechanical ventilation should be provided using the lung protective strategy. To prevent recurrent aspiration, a nasogastric tube is inserted and gastric decompression is performed through either suction or gravity drainage. Quantitative bacteriology using a bronchoalveolar lavage sample obtained through bronchoscopy not only serves as a guide for definitive therapy and de-escalation of antibiotics but can also aid decisions on whether antibiotics should be discontinued if there is no significant bacterial growth [80].
In aspiration pneumonitis, antibiotic therapy is not necessary. However, since it is difficult to distinguish between pneumonitis and pneumonia, it is common practice to use antibiotics with the potential for aspiration pneumonia in mind. In a 2001 survey, the majority of intensivists prescribed antibiotics to patients suspected of aspiration, and 72.4% chose empirical antibiotic regimen over a pathogen specific regimen [81]. The choice of antibiotics can vary based on the local ecology of the ICU. However, it is considered adequate to start with early, empiric, and broad-spectrum antibiotics [82]. Subsequently, during the next 72 hours, the use of antibiotics is de-escalated based on definitive and quantitative culture. In case no significant bacterial growth is observed in the culture, the antibiotics are then discontinued. Based on the bacteriological trend, the use of antibiotics for anaerobic coverage is unnecessary. However, in cases of severe periodontal diseases or evidence of necrotizing pneumonia or lung abscess in computed tomography, the use of antibiotics with anaerobic coverage can be considered [6083].
PREVENTION
Despite proper treatment, aspiration pneumonitis and aspiration pneumonia exhibit high morbidity and mortality; therefore, prevention is crucial. The primary purposes of prevention, for patients with risk factors of aspiration, are to reduce the frequency and amount of aspiration and to minimize the colonization of pathogenic organisms.
General anesthesia is a key risk factor of gastric aspiration, and an opportunity for proactive management and prevention. Fasting prior to the surgery or procedure is one of the key preventive measures to avoid gastric aspiration during general anesthesia. The period of fasting is typically 8 hours as recommended by the American Society of Anesthesiologists (ASA). However, for clear liquids, fasting for longer than 2 h has not shown additional benefits in lowering the risk [8485]. Based on these facts, ASA recommends 2-h fasting for clear liquids for patients of all age groups. The role of fasting when performing sedation for procedures in the emergency department (ED) is controversial. This is because the risk of aspiration during sedation for procedures in ED is thought to be very low, and ED patients are typically healthy without preparation for fasting prior to the admission [86]. Nevertheless, when performing sedation for the procedure, preventive measures, such as adjusting the sedation depth, identifying high risk patients, and monitoring during the procedure, must be considered. The most important intervention to prevent aspiration in inpatients and ICU patients is to position the patients in a semi-recumbent position. Using radioactively labeled gastric contents, it has been found that positioning patients under mechanical ventilation into a semi-recumbent position results in a reduced rate of reflux, thus mitigating the risk of aspiration [8788]. Indeed, the frequency of aspiration was higher in patients in supine position, while the frequency was dependent on the duration of the supine position. In a clinical study comparing the occurrence rate of nosocomial pneumonia in patients under mechanical ventilation, it has been observed that the patient group in semi-recumbent position had significantly lower occurrence rate compared with the patient group in supine position. Furthermore, the difference was more definite in patients receiving enteral feeding [89]. Currently, the semi-recumbent position is a standard practice to prevent aspiration and associated complications.
Dietary intervention has been attempted in patients with dysphasia. The occurrence rate of aspiration pneumonia has been reported to be lower in pseudobulbar dysphagia patients that received mechanical diet with thickened liquids compared with the patients that received pureed diet with thin liquids [90]. However, the occurrence rate of pneumonia was comparable among post-stroke patient groups who were divided into three randomized groups depending on the degree of dietary intervention by a dysphagia therapist [91].
Given that enteric tube feeding increases the risk of aspiration, several attempts have been made to compare different forms of tube feeding to minimize the risk. The most relevant comparison was between gastric and post-pyloric feeding. When considering gastric dysmotility due to a critical illness, gastroparesis, or medication, the post-pyloric feed was thought to be a superior option [92]. However, two randomized prospective clinical studies have reported no difference in the aspiration rates between the two feeding types [9394]. In terms of efficiency to reach the nutritional goal, post-pyloric feed has been considered superior to gastric feeding [9596]. Previous randomized clinical trials have reported no difference in pneumonia complication rate between the nasogastric tube feed and the percutaneous endoscopic gastrostomy tube feed [9798].
Poor oral hygiene increases the risk of aspiration pneumonia. Therefore, oral health care can help prevent aspiration pneumonia by reducing the risk. Currently, the concept of oral health care includes not only oral cleaning but also eating function training. Through oral hygiene management, including oral moisture retention and mechanical cleaning of the tongue and palate, the bacterial burden can be minimized. And improving eating function reduces the occurrence rate of large-volume aspiration [70].
CONCLUSION
Aspiration pneumonitis and pneumonia are acute pulmonary diseases that occur following macroaspiration. Distinguishable characteristics from other aspiration syndromes include rapid progression after large volume aspiration. Although these two diseases are difficult to distinguish clinically, they are two independent disease entities with characteristic pathophysiology. Aspiration pneumonitis is a lung injury from acute inflammation that occurs after chemical burns in the airways and lung parenchyma, while aspiration pneumonia is a pulmonary infection from large-volume aspiration of an infection source. When respiratory or systemic symptoms are observed, supportive care for different symptoms must be immediately provided. Treatment with early, empiric, broad-spectrum antibiotics should be administered then selection of pathogen specific antibiotics or decision to stop or continue the use of antibiotics is made based on quantitative bacteriology.


 XML Download
XML Download