

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Local anesthesia is widely used in dentistry when a dental procedure is expected to be uncomfortable or painful or if the patient cannot tolerate the pain. The advantages of local anesthesia are the anesthetic effect as well as the ability to make the patient more relaxed and less anxious during the dental procedure. Inferior alveolar nerve block (IANB) is commonly used to induce numbness in half of the lower lip, half of the lower teeth, and some areas of the oral mucosa of the mandible on the injected side. This anesthetic technique is used for dental procedures such as cavity preparation and endodontic treatment, and can be supplemented by buccal infiltration anesthesia, if necessary. It is also extensively used for surgical treatments, such as periodontal surgery, dental implantology, extraction, or impacted surgery and apicoectomy, where the use of buccal infiltration anesthesia is more extensive and caudal [1].
Consequently, it is important for a dental practitioner to be familiar with the precise method for injecting and delivering local anesthetics to make the dental procedures more effective and to decrease the complications caused by the injection. However, some dentists do not follow this technique, and this is dependent on their experience and aptitude. In 2001, Keetley and Moles [2] compared the success rates of IANB analgesia among 4 dentists and an experienced dentist. That previous study evaluated the factors that influenced local anesthetic administration, including the practitioner administering the anesthetic, sex and age of the patient, quadrant, reason for local anesthetic, and anesthetic outcome. However, no previous studies evaluated the first injection administered by dental practitioners. Therefore, our study aimed to evaluate the success rate of the first IANB performed by dental practitioners with the goal of improving the dental academic program.
MATERIALS AND METHODS
In this study, we evaluated dental practitioners instead of dental students who practice under the guidance of their advisors. Dental practitioners (n = 106) from Mahidol University who had never carried out or undergone an IANB and had no contraindication or physical issues related to the use of 4% articaine with 1:100,000 adrenaline performed the procedures.
The dental practitioners were divided into 12 groups by randomized control trials. An advisor from the Department of Oral and Maxillofacial Surgery, Mahidol University, was assigned to each group in order to explain the basics of IANB injection.
The dental practitioners were trained in the standard ways to locate the anatomical landmarks for IANB and were instructed how to judge the criteria of a successful IANB procedure. The inclusion criteria and exclusion criteria of the study are shown in Table 1. The data were recorded as described in the following section. This study was approved by the Institutional Review Board of the Faculty of Dentistry/Faculty of Pharmacy, Mahidol University, with a certificate of Exemption (No. MU-DT/PY-IRB 2014/052.1812).
1. Palpation of anatomical landmarks
The dental practitioners were advised to use the index finger for injection on the right side of the patient and the thumb for the left side. In the first step of this procedure, the finger palpates the buccal vestibule at the molar area and continues posteriorly until the external oblique ridge is located. Then, the finger is moved upward along the external oblique ridge, continuing to the anterior border of the mandible, posterior to the second molar. Next, the finger is moved downward to locate the coronoid notch (the deepest depression of the anterior border of the ascending ramus), which is located approximately 6-10 mm above the occlusal plane of the mandibular teeth. From the coronoid notch, the finger is moved medially past the retromolar triangle, then further down to locate the internal oblique ridge. Subsequently, the finger slides buccally to retract the soft tissues and is pulled back at the coronoid notch, such that the pterygomandibular raphe and pterygotemporal space are clearly observed for a depression before the IANB injection.
2. Standard IANB injection technique
A 27-gauge needle (30 mm) and self-aspirating syringes with a local anesthetic solution (4% articaine with adrenaline 1:100,000 [1 cartridge = 1.7 ml]) were used. The standard IANB technique was followed [345]. The anesthetic was injected into the pterygomandibular space, while the axis of the syringe barrel was parallel and was placed on the occlusal surfaces of the mandibular teeth. The needle penetrated 2 cm into the soft tissue until it approximated the bone around the mandibular foramen, as detected by tactile sensation (Fig. 1).
We evaluated the local anesthetic that remained after IANB, landmarks located, side of injection, finger used for retraction, injection position, and parallelism of the dental syringe to the lower occlusal plane. The subjective and objective onsets, duration of anesthesia, and associated complications were also noted, and the pain score was evaluated by using a visual analog scale (VAS). The success of the IANB procedure was evaluated by stimulating the labial mucosa attached around the lower canine tooth on the injected side with a sharply tipped dental explorer at a force of 200 mN (20 g) [67]. If the area was successfully anesthetized, the probing did not elicit any pain stimulus. Only 1 anesthetic cartridge was permitted per dental practitioner.
The subjective onset of anesthesia in the patient after drug delivery was recorded at 4 time points: no numbness, 0 min; good onset, more than 0 to 5 min; acceptable onset, more than 5 to 10 min; and subjective onset failure, more than 10 min. The duration was divided into each group every 60 minutes, and 0 minutes represented an absence of numbness.
RESULTS
In this study, 106 IANB analgesic procedures were performed, but 11 cases were excluded because of inadequate data collection. Consequently, the results from the IANB procedures of 95 dental practitioners were used for data analysis. IANB failure according to the type of technique used by the dental practitioners and the localization of landmarks is shown in Table 2.
The side of injection and the finger used to check for retraction are shown in Fig. 2. The right side was used for injection by 65 dental practitioners. Only 3 dental practitioners injected the local anesthetic in the incorrect patient position. Five dental practitioners handled the barrel of the syringe incorrectly, without placing it parallel to the occlusal plane of the mandibular teeth.
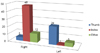
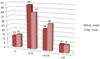
The amount of local anesthetic that remained after IANB injection is shown in Fig. 3, and the subjective and objective onset periods according to the ranges described in the previous section are shown in Fig. 4. In the majority of cases, the duration of anesthesia was from 180 to 360 min (Fig. 5). The complications found in this study were one case each of numbness at the ear, sharp tongue pain, muscle pain, and hyperventilation. The average pain score (VAS) was 2.5 ± 1.85 during needle insertion and 2.1 ± 1.8 during consecutive administration of local anesthetic, while the average patient excitement score was 4.9 ± 2.4.
DISCUSSION
Most of the dental practitioners in this study (81/95 or 85.26%) used the method mentioned above to palpate and locate the anatomical landmarks. This method is easy to follow and helps the practitioner to locate the acceptable area for delivery of local anesthetic, which adds to the success of IANB. Moreover, 68.42% of the dental practitioners (65/95) were right-handed, so most of them injected on the right side. This also affected the finger that the dental practitioners used to retract the subject's cheek before the injection. Dental practitioners who injected on the right side tended to use the left index finger to retract the cheek, while dental practitioners who injected on the left side were more likely to use the left thumb for retraction. The simplest explanation for the different preferences for using the finger or thumb is that the practitioner used the digit that was more convenient.
Approximately 0-0.3 ml of local anesthetic remained after IANB for most dental practitioners (71/95 or 74.74%). The remaining local anesthetic was further used for buccal nerve block. More anesthetic was provided if the dental practitioners had no remaining local anesthetic for the buccal nerve block. The onset was approximately 0-5 mins for nearly half of the dental practitioners in this study (45/95 or 47.37% for subjective and 41/95 or 43.16% for objective onset), with the use of 4% articaine with 1:100,000 adrenaline. This finding is consistent with that of the study by Kambalimath et al., who reported a subjective onset of 1.35 min and an objective onset of 2.12 min [8]; other studies reported onsets of 4.2 ± 2.8 min [9], 149.5 ± 14.29 sec [10], 53.03 sec (0.93min) [11], and 1.66 ± 0.13 min [12]. The average duration of IANB was approximately 240-300 minutes (35/95 or 36.84%) after the initiation of numbness. This result was similar to those of Sierra et al. [11] and Gregorio et al. [12], who reported durations of 273.8 ± 15.94 min and 220.8 min, respectively. Meanwhile, the duration of anesthesia was longer than those reported by Moore et al. [9] and Colombini et al. [10] (61.8 ± 59 min and 51.2 ± 55.9 min, respectively).
We observed each of the following complications in one case: numbness at the ear, sharp tongue pain, muscle pain, and non-severe hyperventilation. Other IANB failures were also found in our study, including complete absence of numbness or delayed subjective and objective onset of anesthesia. We found that correctly performing IANB injection by following the standard technique could prevent incorrect local anesthetic injection and postoperative complications, and this finding is relevant to both dental education and patient practice.
According to Keetley and Moles [2], the skill of the dental practitioner is one of the key factors associated with anesthesia failure; however, we found many other influential factors in this study, such as the advisors, dental practitioner, injection technique, and patient.
In conclusion, the only recorded factor that affected the success of local anesthesia was the skill of the dental practitioner. This reinforces the notion that local anesthetic injection, especially IANB, is a technique-sensitive procedure.





 XML Download
XML Download