

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Knowing the kinds and frequency of emergencies during dental treatment helps prepare for possible emergencies. However, the available research on these emergencies has been mostly based on surveys, which are ineffective in producing quality data due to low response rates and memory errors [123456].
At the Seoul National University Dental Hospital, the Department of Dental Anesthesiology is a designated emergency response team responsible for the primary care of emergencies in the hospital, as the Dental Hospital is located apart from the general medical center (Fig. 1). Having an emergency response team reduces the likelihood of cardiac arrest and the mortality rates [78910], and facilitates the systematic collection and management of data on emergencies. While this study used data from a single hospital, it nevertheless enables comprehensive research on the emergencies that can arise during the treatment of outpatients, as it is not based on surveys but on mandatory records.
This research used the 10-year records of the Seoul National University Dental Hospital to study the instances in which the Department of Dental Anesthesiology was called to handle emergencies in the course of dental treatment.
The study aims to contribute to hospitals' preparedness for dental treatment by providing a systematic analysis of the kinds and frequencies of emergencies during dental treatment, and the responses and results that have been made in such emergencies.
SUBJECTS AND METHOD
1. Research Subjects
The subjects of this study were 35 patients from the records of emergencies handled by the Department of Dental Anesthesiology (Emergency Response Team) during the dental treatment of outpatients over a 10-year period (from November 1, 2004 to November 30, 2013). The emergencies that arose in large operating theaters and inpatient rooms, as well as those that concerned medical personnel including interns, residents, and medical professors, were excluded. Details from the emergency records and patients' medical records were extracted for study and analysis.
2. Research Method
The research was approved by the Institutional Review Board of the Seoul National University Dental Hospital (ID: S-D20140037), and was conducted on 35 patients. The following information was reviewed: the emergency rate; department in which the emergency happened; occurrence time; kind of emergency; and response result. The clinic's emergency record chart was used as the data source for the research. Incomplete records were excluded.
The emergency rate was calculated according to the total number of outpatients in the hospital over the last ten years. The patients who had experienced emergencies were categorized according to their age and gender, with the age divided into decades. To categorize the departments in which the emergencies had occurred, the patients' registered departments and medical records were referred to. The time of the emergency occurrence was categorized according to the different stages of treatment: before treatment; during treatment; after treatment; after local anesthesia; and during or after CT-taking. "During treatment" represented the time from when the patient sat in the examination chair until he or she got up from the chair. The kinds of emergencies were categorized as: syncope; dizziness; seizure; anaphylaxis; cardiovascular dysfunction; airway obstruction; ingestion of foreign body; anxiety; and nausea or vomiting. If multiple symptoms were present, the most prominent symptom reported to the Department of Dental Anesthesiology was selected. The response outcome was categorized by "transferred to emergency room", "sent home after treatment", or "hospitalized in dental hospital".
RESULTS
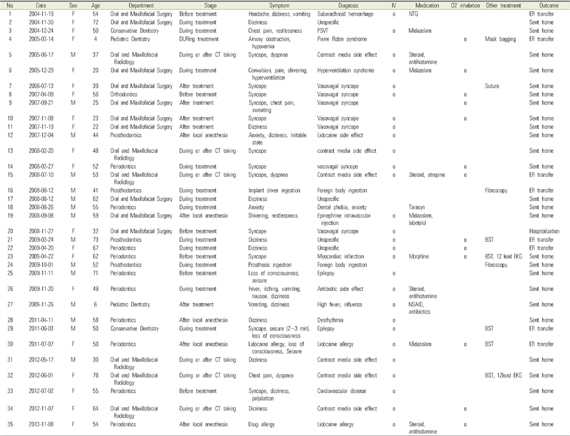
Appendix 1 lists the emergencies that took place over the 10-year period.
1. Analysis of subjects
Over the 10-year period, the Department of Dental Anesthesiology was called to handle 35 emergency cases. The total number of outpatients at the Seoul National University Dental Hospital was 2,890,424, and the Department of Dental Anesthesiology was therefore called to deal with emergencies for 0.12 cases per 10,000 outpatients (0.0012%). Table 1 shows the gender ratio for the emergency cases: 20 women (57.1%) and 15 men (42.9%). In terms of age, 2 patients (5.7%) were aged 0-9; 4 patients (11.4%) were aged 20-29; 4 patients (11.4%) were aged 30-39; 4 patients (11.4%) were aged 40-49; 4 patients (11.4%) were aged 50-59; 13 patients (37.1%) were aged 50-59; 4 patients (11.4%) were aged 60-69; and 4 patients (11.4%) were aged 70-79.
2. Department in which emergency occurred
Among the 35 cases of emergencies in which the Department of Dental Anesthesiology was involved, 10 cases (28.6%) occurred in the Department of Periodontics; 10 cases (28.6%) in the Department of Oral and Maxillofacial Surgery; 6 cases (17.1%) in the Department of Oral and Maxillofacial Radiology; 4 cases (11.4%) in the Department of Prosthodontics; 2 cases (5.7%) in the Department of Conservative Dentistry; 2 cases (5.7%) in the Department of Pediatric Dentistry; and 1 case (2.9%) in the Department of Orthodontics (Table 2).
The number of emergencies per 10,000 outpatients in each department over the 10-year period was as follows: 0.208 cases in the Department of Periodontics (0.0021%, 10 out of 480,948); 0.201 cases in the Department of Oral and Maxillofacial Surgery (0.0020%, 10 out of 497,603); 0.056 cases in the Department of Oral and Maxillofacial Radiology (0.0006%, 6 out of 1,069,346); 0.132 cases in the Department of Prosthodontics (0.0013%, 4 out of 303,928); 0.058 cases in the Department of Conservative Dentistry (0.0006%, 2 out of 347,820); 0.064 cases in the Department of Pediatric Dentistry (0.0006%, 2 out of 313,629); and 0.035 cases in the Department of Orthodontics (0.0003%, 1 out of 289,479).
3. Time of emergency
Table 3 shows the time or stage of treatment at which the emergency arose. Out of the 35 cases, 6 cases (17.1%) occurred before treatment; 13 cases (37.1%) occurred during treatment; 5 cases (14.3%) occurred after treatment; 5 cases (14.3%) occurred following local anesthesia; and 6 cases (17.1%) occurred during or after CT-taking.
4. Emergency symptoms
Table 4 categorizes the 35 emergency cases according to the patients' symptoms: 10 cases (28.6%) involved syncope; 9 cases (25.7%) involved dizziness; 3 cases (8.6%) involved seizure; 3 cases (8.6%) involved anaphylaxis; 2 cases (5.7%) involved cardiovascular dysfunction; 2 cases (5.7%) involved airway obstruction; 2 cases (5.7%) involved ingestion of a foreign body; 2 cases (5.7%) involved anxiety; and 2 cases (5.7%) involved nausea or vomiting.
5. Diagnosis and treatment of emergency patients
The emergency response team based its diagnosis and treatment on the patients' symptoms. All patients' vital signs were monitored. An IV line was placed in 28 patients. 12 patients were administered drugs such as ketorolac, steroids, antihistamines, nitroglycerin, nonsteroidal anti-inflammatory drugs, antibiotics, morphine, midazolam, and labetalol. 12 patients were put on oxygen inhalers. Other treatments included suture, endoscopy, blood sugar tests, and 12-lead cardiograms.
6. Treatment outcome
Table 5 shows the outcomes of the emergency treatments. Following treatment, 26 patients (74.3%) recovered and were sent home. 8 patients (22.9%) were transferred to an emergency room in the General Hospital, while one patient (2.9%) was hospitalized in the Dental Hospital. There were no fatalities.
CONCLUSION AND DISCUSSION
A number of studies have previously considered the kinds of emergencies occurring in the course of dental treatment, and how to respond to them. In England, 1,500 dental practitioners were surveyed on the emergencies arising during dental treatment, and similar studies have also been conducted in Germany and Japan [1234]. Moreover, studies have also been conducted on the emergency situations arising in the course of dental treatment in dental teaching hospitals [56].
However, past studies presented a clear limitation in that they were based on surveys. While the response rate in each study was different, as not all of those surveyed answered, the collected data may have caused distorted representations. Moreover, surveys are subject to inaccuracies as they depend on human memory. To solve this intrinsic problem with surveys, one study conducted separate analyses of the cases in which the respondents had said that they could remember accurately, and those in which they had said that they could not [6]. However, this method did not get rid of the limitation entirely. Furthermore, in the teaching hospitals, multiple respondents redundantly reported the same emergencies. These limitations have been calling for research based on accurate records, rather than on surveys dependent on memory.
The Seoul National University Dental Hospital is separate from the General Hospital, and is responsible for the primary care of emergencies arising at the Dental Hospital. Therefore, data on emergencies and emergency management are collected systematically. Although this study used data from a single hospital, it nevertheless enabled comprehensive research on the emergencies that can arise during the treatment of outpatients, as it was not based on surveys but on mandatory records. This research reviewed the emergencies that occurred in the course of dental treatment at the Seoul National University Dental Hospital over a 10-year period, based on the records of the emergencies for which the Department of Dental Anesthesiology was called. The total number of dental treatments over the period was 2,890,424. With these data, the limitations caused by skewed survey response rates and memory errors were eliminated.
The total emergency rate represented 0.12 cases per 10,000 patients, a much lower ratio than in a previous study, which had reported an emergency rate of 2.9 cases per 10,000 patients [2]. First, this significant discrepancy could be attributed to an overrepresentation of patients in this study from the redundant counting of patients who had visited multiple departments in the hospital. Second, there may have been cases in which the practitioner in charge handled the emergency without calling the Department of Dental Anesthesiology. Third, the past study may have featured survey errors. In a study by Girdler NM and Smith DG [2], the survey response rate was low, at 34.0%. However, the practitioners who had experienced emergencies may have been more willing to respond, resulting in a response rate discrepancy.
As per Table 2, the Departments of Periodontics (10 cases), Oral and Maxillofacial Surgery (10 cases), and Oral and Maxillofacial Radiology (6 cases) showed the most frequent emergencies. The high frequency of emergencies in the Departments of Periodontics and Department of Oral and Maxillofacial Surgery may be attributed to the departments' frequent extractions and oral surgeries after anesthesia. Out of the 5 emergencies related to local anesthesia, 3 cases occurred in the Department of Periodontics. Among the emergencies that occurred in the Department of Oral and Maxillofacial Surgery, 6 cases were related to extraction, incision and drainage, and biopsy. A past study has shown that syncope is most common in the departments that often involve surgeries [6].
All 6 cases of emergencies in the Department of Oral and Maxillofacial Radiology were side effects of the contrast agents in CT. The past studies were conducted on medical practitioners, and the emergencies related to radiology were not frequent. This result suggests that the dental clinics that use CT need to be aware of the possible emergencies arising from the side effects of contrast agents.
Compared to the study conducted in Japan, the number of emergencies from pulpectomy was small. According to Matsuura H [4], 26.9% of the emergencies in the prior study were related to pulpectomy, but no such emergency was reported in this research.
Table 3 shows the stage at which the emergency occurred. 13 emergencies arose during treatment, and, with the inclusion of the 5 cases related to local anesthesia, a total of 18 emergency cases occurred after initiation of the treatment. Past studies have shown similar results, with the highest number of emergencies arising during treatment [14]. 5 cases (14.3%) were related to local anesthesia, a slightly lower rate than the 54.9% [4] and 16.4% [1] found in past studies. To explain these differences, some cases may have been simply recorded as "during treatment" without providing specific details, making for incompleteness in the records.
Table 4 shows the emergency patients' symptoms. As found in prior studies [125,11], syncope (28.6%) was the most common symptom.
In this research, no fatality was recorded over the 10-year period. However, a previous study showed that 0.013 cases of fatalities occurred per 10,000 patients in England and Scotland [1]. The absence of fatalities can be attributed to the low emergency rate, as compared to the emergency rates in other studies. Moreover, while the percentage of cases in which the patients were transferred to the emergency room after emergency treatment (20.0%) was similar to that in other studies (20.0% [4] and 23.0% [1]), the transfers were made swiftly, preventing aggravation of the cases. Prior studies have shown that operating a designated emergency response team reduces the number of critical emergencies [78910]. This research attributes the absence of fatalities to the designated emergency response team of the Seoul National University Dental Hospital.




 XML Download
XML Download