

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The mandibular molar region is difficult to anesthetize with infiltration anesthesia. This is because its dense bone tissue makes it hard for an anesthetic to infiltrate the area. Localized inflammation also reduces the effectiveness of infiltration anesthesia by lowering the pH, thus decreasing the available amount of free base-type anesthetics [12]. In contrast, conduction anesthesia (nerve block) of the mandibular foramen provides effective anesthesia of this area, by acting directly on the nerves that run through the pterygomandibular space. Furthermore, when using nerve block techniques, the anesthetic is administered directly to the central nervous system, making this method less susceptible to the effects of local inflammation. Mandibular foramen nerve block is therefore an extremely effective method of molar anesthesia. However, during conventional nerve block (the conventional technique; CT), the tip of the needle is inserted as close as possible to the inferior alveolar nerve, leading to a high risk of nerve damage. As an alternative, Takasugi et al. suggested the use of a proximal nerve block (the anterior technique, AT), in which the tip of the needle is placed as far as possible towards the oral side of the pterygomandibular space [3]. In this way, the needle is distant from the inferior alveolar nerve, so the risk of causing nerve damage is lessened. In addition, a very fine needle can be used because of the shallow insertion depth, thereby reducing the pain felt by patients [3].
Generally, epinephrine-lidocaine (EL) is used for nerve block when performing the CT, but epinephrine causes elevated blood pressure and tachycardia. Thus, the dose of epinephrine must be as low as possible when administering local anesthesia, especially in patients with circulatory disorders. In contrast, the vasoconstrictor felypressin enhances the effect of local anesthetics without affecting the heart [4]. Indeed, the combination of felypressin and propitocaine (FP) is widely used as a local anesthetic for patients with circulatory disorders. Hypothetically, proximal nerve block using FP and the AT could induce anesthesia with no effect on heart function, and with a low risk of nerve damage. However, this combination has not been tested during mandibular anesthesia for dental procedures.
The present study compared the efficacy and safety of an AT nerve block using FP with a CT nerve block using EL in healthy subjects, by analyzing anesthetic success rate, duration, and injection-mediated pain. The experimental design addressed the first incisor, premolar, and molar of the right mandible independently, for possible asymmetry in anesthetic responses.
MATERIALS AND METHODS
1. Subjects
The subjects comprised 40 ASA Grade 1 students recruited at our dental university school. The exclusion parameters were: age < 18 years, dental procedures in the past 3 months, or any medication that may have affected the response to anesthesia. This study was approved by the Ethics Committee of our university school and was performed in accordance with their guidelines and the guidelines of the Declaration of Helsinki. All subjects provided their written informed consent upon sufficient understanding of the purpose and objective of the study.
2. Methods of anesthesia
The 40 subjects were randomly assigned to two treatment groups of 20 subjects each, according to the type and position of anesthesia: right CT or right AT. The effects of each anestheticprocedure were measured on the mandibular lateral incisor, mandibular first premolar, and mandibular first molar. The exclusion factors for individual teeth were: (1) nonvital, (2) untreated caries, or (3) a MOD inlay or more significant restoration. If any of the three teeth in each patientwas excluded, the test was conducted instead on the central incisor, second premolar, or second molar located on the same side.
All the anesthetic operations were carried out by the same dental anesthesiologist, and the subject was not told which method had been used. The anesthesiologist carried out the procedures while standing on the right side of the patient.
2.1. Conventional nerve block technique
The subject was immobilized in the seated position so that the mandibular occlusal plane was parallel with the floor when the mouth was opened maximally. A 27 G, 21 mm dental disposable syringe needle was inserted 1 cm above the mandibular occlusal plane, in the depression between the internal oblique line and the pterygomandibular fold. The needle was inserted to a depth of 20 mm from the opposing first premolar, with the bevel facing the bone. After a negative suction test had been confirmed, 1.8 ml ofEL (2% lidocaine containing 1: 80,000 epinephrine) was administered over 1 min [5].
2.2. Anterior nerve block technique
The body posture and insertion point were the same as for the CT. However, for the AT, a 33 G, 12 mm dental disposable syringe needle was inserted to a depth of 12 mm from the opposing first molar, with the bevel facing the bone. After a negative suction test had been confirmed, 1.8 ml of FP (3% propitocaine containing 0.03 IU/ml felypressin) was administered over 1 min.
3. Measurement of anesthetic effects
3.1. Anesthesia success rate
(i) After the teeth concerned had been protected against moisture with cotton wool rolls and gauze and thoroughly dried, the probe of a Digitest electric tooth vitality tester (Parkell Inc., USA) with the tip smeared with electrocardiography gel was placed in contact with healthy enamel at a point midway between the incisal and gingival margins.
(ii) The stimulus strength was increased from 0 to a maximum of 64 over a 20-s period. The value at which the subject felt pain was taken as the threshold value. Measurements were performed twice for each tooth, and the mean value was calculated as the final measured value for each tooth.
(iii) The pain threshold was measured at 5-min intervals, from 5 min to 60 min after the anesthetic injection.
(iv) The absence of a response to the maximum stimulus was defined as "successful anesthesia."
(v) The anesthesia success rate for each tooth concerned was calculated by dividing the number of subjects for whom successful anesthesia was achieved by the total number of subjects.
(vi) The pre-anesthesia value was considered the base threshold value. If the pain threshold had not increased within 10 min after administration, this was considered unsuccessful anesthesia and measurement was terminated.
3.2. Anesthesia duration
The anesthetic effect was considered to be manifested when the subjects experienced a paralysis sensation in the lower lip. Sensation in the subjects' lower lips was checked at 15-min intervals, and the duration of action was taken as the time from the induction of anesthesia to the time when the anesthetic effect had worn off. This was not measured in subjects for whom anesthesia was unsuccessful.
RESULTS
There were no significant differences on the right side between those subjects who underwent the CT versus those who underwent the AT in terms of age or sex (Table 1).
1. Anesthesia success rate
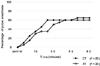
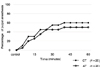
The success rate after 60 min was 65% for the CT and 60% for the AT at the first molar, 65% for the CT and 60% for the AT at the first premolar, and 60% for the CT and 50% for the AT at the lateral incisor (Figs. 1,2,3). There were no significant differences between the success rates of the CT versus the AT at any tooth.
2. Duration of action
The two nerve block techniques were compared in terms of duration of anesthesia based on lip numbness. The duration of action was significantly shorter for the CT (233 37.5 min) than for the AT (267 37.2 min; P < 0.05) (Table 2). These results show that the AT provides a longer duration of anesthesia than the CT.
3. Pain from anesthetic administration
For the CT, pain upon administration of anesthesia was most often rated as 1 on the 0-3 scale described above, followed by 2. For the AT, it was most often rated as1, followed by 0, on the same 0-3 scale. There was no significant difference between the groups (Table 3). No subject in either group complained of difficulty in opening their mouth after the procedure.
DISCUSSION
In the current study, there was no significant difference between the 60-min success rates of the CT versus theAT at any of the three teeth examined. Furthermore, Takasugi et al. reported success rates of 60% for the AT using FP and 62% for the AT using EL for the first molar [3]. This suggests that the AT is equally as effective as the CT as a method of anesthesia, even when using EL rather than FP.
The anesthetic administered during infiltration anesthesia infiltrates the bone to reach the nerves, and is absorbed by the surrounding blood vessels at the same time. Reduced blood flow at the administration site thus prolongs the localization of the anesthetic, enhancing its effect and extending the duration of action. Therefore, a vasoconstrictor is added to most dental local anesthetics in order to reduce blood flow. Epinephrine acts on 1 receptors causing vasoconstriction, but also stimulates β receptors to increase cardiac function. The dose of epinephrine given should therefore be as low as possible when administering local anesthesia for patients with circulatory disorders [6]. Felypressin is a vasopressin analog that constricts the blood vessels without affecting the heart and is therefore widely used for patients with circulatory disorders. However, its vasoconstrictive action is weak compared to that of epinephrine [4], so it prolongs the localization of anesthetic to a lesser extent. In infiltration anesthesia, the action of FP therefore appears later and lasts longer than that of EL, meaning that a double dose of EL is required to achieve the same duration of effect [78]. However, during mandibular foramen nerve block, anesthetic administered into the pterygomandibular space infiltrates the connective tissue to reach the inferior alveolar and lingual nerves. Since connective tissue is infiltrated more easily by anesthetic than bone, the use of a vasoconstrictor is less important. This may be the reason for the absence of significant differences between the success rates of the CT and AT.
Nordenram et al. [9] compared the administration of FP and EL for infiltration anesthesia of the maxillary incisors. While EL had a longer duration of action on the tooth pulp, the duration of action of FP and EL on the lips was similar. Petersen et al. [10] also found that EL had a longer duration of action in infiltration anesthesia, but a similar duration to FP when used for nerve block. These findings show that the duration of action is not affected by the vasoconstrictor if the anesthetic is not required to infiltrate the bone. When Padfield [11] administered propitocaine and lidocaine to the skin of the forearms of volunteers and compared the results, he found that propitocaine had a significantly longer duration of action. In the present study, we found that the AT had a longer duration of action compared to that of the CT, which suggested that the duration of action of nerve block may be more strongly influenced by the properties of the specific anesthetic used than by those of the vasoconstrictor.
Although this experiment did not show a significant difference in pain upon anesthetic administration between the two groups, the results are nevertheless important. The AT used a fine, short needle, whichinduced less pain than that used in the CT. Since the majority of cases of vasovagal reaction or hyperventilation occur during the administration of local anesthesia, reducing the associated pain is important for preventing systemic complications.
One limitation of the current study is that we did not measure the anesthetic action on the lingual nerve. Anesthesia of the floor of the mouth and tongue is often essential for oral surgical treatments. Our results, however, do not show whether the AThas an equivalent success rate to that of the CT with respect to the lingual nerve. Another issue involves using patient reaction to an electric pulp stimulus as an indicator of the anesthetic effect, rather than investigating the anesthetic effect on dentine or bone. Clinical studies will be required in the future to confirm the overall value of the AT.
Our study suggests that the AT is a method of anesthesia with an equivalent success rate to that of the CT, but with a longer duration of action and less initial pain on injection.




 XML Download
XML Download