

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Extubation of a nasotracheal tube after oral and maxillofacial surgery can sometimes be a serious challenge. An acute airway obstruction can occur immediately following extubation because of edema or a hematoma formed within the oral cavity. Deformation of head and neck structures can directly influence airway maintenance and result in a complete loss of function depending on the severity [1]. Furthermore, increasing the occlusal stability can cause airway obstruction in patients with trismus or iatrogenic restriction of mouth opening. In these cases, performing an endotracheal intubation is not straightforward and may not be possible. When maintaining the airway is expected to be difficult after extubation, a tracheotomy or a delayed extubation is likely to be performed. However, unexpected dyspnea after extubation can be fatal.
In this situation, tracheal intubation can be very difficult or nearly impossible. When a patient encounters dangerous situations, a tracheotomy should be performed. It is difficult to execute a tracheotomy as a standard emergency procedure because it is challenging and poses complications [2].
We report a case of airway obstruction following extubation in a patient who underwent two-jaw surgery. The airway obstruction was well controlled with a Combitube (37 Fr, Mallinckrodt, USA) without specific complications (Fig 1).
CASE REPORT
The patient was a 24-year-old man (178 cm/67 kg) who had no specific underlying medical problems. He was scheduled for two-jaw surgery as a result of malocclusion. With the use of facial computer tomography, it was determined that the patient had an upper airway obstruction that extended from the pharynx to the larynx. After arriving in the operating room, the patient was monitored with a bispectral index, an electrocardiogram, an automated noninvasive blood pressure device, and pulse oximetry. For the induction of anesthesia, an intravenous injection of propofol (120 mg) and rocuronium (50 mg) was used. Nasotracheal intubation was performed with no specific difficulties. Arterial cannulation was performed via the dorsalis pedis artery for monitoring arterial blood pressure and performing a blood test. Additionally, a 16-gauge cannula was placed in the great saphenous vein for venous cannulation. Total intravenous anesthesia was maintained using propofol and remifentanil. During surgery, no special events occurred and the vital signs and oxygen saturation of the patient were normal.
The total operation time was 5 hours and 50 minutes. The total anesthetic time was 6 hours and 40 minutes. The total fluid input was 2000 mL (crystalloid) and 1000 mL (colloid). The estimated blood loss was approximately 800 mL and the total urine output was 1700 mL.
After the operation was finished, pyridostigmine bromide (15 mg) and glycopyrrolate (0.4 mg) were administered for the reversal of muscle relaxation. Intraoral blood and secretions were sufficiently suctioned. Following the return of regular spontaneous breathing and a fair recovery of the patient's level of consciousness, he was transferred to the post-anesthesia care unit—(PACU) in the Semi-Fowler's position—with a nasotracheal tube in-situ.
While in the PACU, the patient maintained a regular respiration rate with a T-piece while still in the Semi-Fowler's position. Oxygen saturation was maintained at 100% with the administration of oxygen at a rate of 5 L/min. Thirty minutes later, the surgeons requested extubation. The patient was in a bimaxillary fixation state with a wafer. The anesthesiologist ensured that the patient was conscious and observed as the patient performed a head lift for more than 5 seconds and fully grasped with hands. A hematoma secondary to bleeding from both jaws was confirmed by a hand examination.
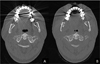
After deep breathing, extubation was conducted and an oxygen mask was applied immediately with oxygen administered at a rate of 5 L/min. At that moment, the patient complained of respiratory difficulty, even though the anesthesiologist lifted the patient's chin. Despite untying the bimaxillary fixation and ambubagging, the oxygen saturation fell below 90%; thus, the patient called a team member for help. As a result of a narrow mouth opening (about 1 cm), an emergency airway was obtained by inserting a Combitube (37 Fr, Mallinckrodt). Oxygen saturation rose to 100% and the patient regained regular respiration (Fig. 2). An emergency operation was deemed necessary on the suspicion of a bleeding problem; thus, the Combitube was exchanged for a nasotracheal tube with a fiberoptic endoscope. It was confirmed that the breathing difficulty was not due to bleeding. The operation to verify a bleeding problem lasted 2 hours and 30 minutes. The patient was transferred to the intensive care unit in the oral surgery unit with a nasotracheal tube in-situ. The following day, a facial computer tomography was taken to verify airway space (Fig. 3). We observed that the airway space narrowing was severe compared to its pre-operational state. The patient's state was examined in the PACU for extubation. Tongue thrust and head lift were normal after the bimaxillary fixation was untied. After the swelling subsided, the patient was successfully extubated without complications.
DISCUSSION
After two-jaw surgery, the position of the mandible changes to a retruded position, such that a posteroinferior movement of the tongue occurs. This affects the width of the airway space. This change is more significant in the oropharynx and the hypopharynx than in the nasopharynx. Previous results from short-term studies show an increase in the nasopharynx and a decrease in the hypopharynx after operation. However, in long-term follow-up studies, there are no statistically significant changes [34]. After protruding the maxilla, the extent of the mandibular shift to the retrude position decreases compared to simply retruding the mandible. This results in expansion of the upper respiratory space [5]. Furthermore, two-jaw surgery causes the tongue to move in a posteroinferior direction and also causes the hyoid bone to move in an inferior way. This causes a physiologic reflex to maintain the airway after two-jaw surgery [6]. This also affects safety after surgery.
Single mandibular surgery has been found to result in a considerable decrease in the sizes of the oropharynx and hypopharynx. However, it has been widely accepted that posterior movement of the mandible after two-jaw surgery causes obstruction of the airway space and a decrease in the size of the hypopharynx [6], which is affected by anterior movement of the soft palate and velopharyngeal muscle [7]. Likewise, soft tissue swelling after surgery—and changes in soft tissue due to intubation—narrow the airway space directly after surgery. In all these regards, especially for patients with pre-existing narrow upper and lower airways, respiratory problems occur more frequently.
In particular, patients who undergo orofacial surgery commonly experience a difficult intubation because of deformities, bleeding, or edema in the orofacial area, as well as difficulty with achieving a tight application of the facial mask. Edema of the respiratory tract can cause obstruction of the airway and lead to difficult intubation, which threatens the patient's safety. A tracheostomy can be performed in an emergency airway situation. However, the risks and complications of a tracheostomy should not be overlooked and it cannot be used as a routine procedure.
In our reported case, we called for help and tried a chin lift to maintain the airway, but it was insufficient. In such situation, one can intubate using a laryngoscope or supraglottic airway devices to maintain the airway [8]. The use of a laryngoscope prior to two-jaw surgery can damage the surgical site. Moreover, in a bimaxillary fixation case, one should untie the fixation to maintain airway space.
Also, based on the clinical situation, one can choose to use a bronchofiberscope, a light wand, retro-endobronchial intubation, a laryngeal mask or a Combitube [9]. Furthermore, a laryngeal mask can be used to guide intubation in cases of difficult endotracheal intubation. A Combitube, light wand, or a laryngeal mask is especially useful in difficult situations in order to obtain proper endotracheal intubation. In the present case, we used a Combitube, which was successful in supplying oxygen to the patient.
A Combitube is composed of dual tubes and can be inserted into the esophagus or trachea without using a laryngoscope. It can easily maintain the airway, whether it is inserted into the esophagus or the trachea [9]. Normally without a laryngoscope, a Combitube inserts into the esophagus in more than 80% of cases. The Combitube has two tubes. The first should be obstructed in cases where it is inserted into the esophagus. There are many small pores on that tube so that oxygen can flow into the trachea. The other tube is used in cases where it is inserted into the trachea. The end of that tube is open so when it is ventilated, oxygen supply is possible. For adults, there are two sizes: 37 F (height between 120 and 167 cm) and 41 F (height more than 167 cm). Smaller sizes are used for children.
The Combitube is simple to insert. First, insert the Combitube along the curve of the airway while extending the patient's neck. The insertion depth is confirmed when the circle on the tube is located on the patient's teeth. Second, puff out the blue and white cuff as described above. If there is no air sound in the upper abdominal region and one can see the chest rising after attaching the bag-valve to the blue tube, then the Combitube was inserted appropriately into the esophagus. If there is an air sound and no chest rising is observed, then the Combitube was inserted into the trachea. In our reported case, we could hear an air sound from the blue tube and there was no chest rising. Thus, we believed the Combitube was in the trachea; therefore, we attached the bag-valve to the white tube, and finally confirmed that oxygen was adequately administered into the trachea.
In conclusion, the Combitube can be easily applied and has few complications. Therefore, it can be used as an alternative for patients who experience emergency breathing problems that occur because of structural deformation of the soft tissue and edema after two-jaw surgery and insufficient mask ventilation.


 XML Download
XML Download