

This article has been corrected. See "Erratum: Can We Omit Intraoperative Frozen Section According to the Result of the Preoperative Fine-needle Aspiration Cytology of a Thyroid Nodule?" in Volume 16 on page 56.
 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Fine needle aspiration (FNA) is a useful preoperative diagnostic tool for thyroid nodule because of the high sensitivity and specificity. The aim of this study is to determine the necessity of intraoperative frozen section (IOFS) after fine needle aspiration.
Methods
Data of 534 patients with a single thyroid nodule who underwent thyroidectomy from June 2006 to August 2013 were reviewed retrospectively. FNA was performed preoperatively in all patients and IOFS was performed selectively according to the intraoperative findings and FNA results. The sensitivity, specificity, positive predictive value, negative predictive value and accuracy of FNA and IOFS for malignant nodules were analyzed.
Results
The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of FNA for malignant nodules were 100%, 95.5%, 99.8%, 100%, and 99.8%, respectively. All nodules diagnosed as benign by FNA were reaffirmed as benign nodules by permanent sections. When the result of FNA was suspicious for malignancy, specific features of preoperative ultrasound, including hypoechoic, size<10 mm showed high positive predictive value and accuracy (98%, 86.9%, and 100%, 78.7% respectively).
Conclusion
Performance of IOFS was not necessary when the result of FNA was consistent with malignancy or benign. However when the result of FNA was non-diagnostic or atypia, IOFS should be performed for more accurate detection of malignancy. When the result of FNA is suspicious for malignancy, IOFS is restrictively useful for excluding benign nodules using the features of ultrasound. In addition, IOFS is not useful in finding malignant thyroid nodules when the result of FNA is follicular neoplasm.
Figures and Tables
 | Fig. 1Flow chart for the diagnosis of a single thyroid nodule. Suspicious features include hypoechoic, heterogeneity, ill-defined margin, microcalcification, taller-than-wide and solid, FNA = fine needle aspiration; IOFS = intraoperative frozen section; US = ultrasound.
|
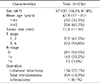
Table 1
Clinicopathological characteristics of patients who underwent operation for a single thyroid nodule
![]()


Table 4
Correlation of fine needle aspiration and frozen section with final histologic findings

NH = Nodular hyperplasia; FC = Follicular carcinoma; FA = follicular adenoma; PTC = Papillary thyroid carcinoma; UC = undifferentiated carcinoma; FNA = fine needle aspiration; IOFS = intraoperative frozen section. *Other benign includes Chronic lymphocytic thyroiditis with oncocytic cells, granulomatous thyroiditis, fibroinflammatory lesion, lymphocytic thyroiditis, hyalinizing trabecular tumor.
![]()
Table 5
Sensitivity, specificity, positive predictive value, negative predictive value and accuracy of fine needle aspiration and intraoperative frozen section for a single malignant thyroid nodule

![]()

References
1. LiVolsi VA, Baloch ZW. Use and abuse of frozen section in the diagnosis of follicular thyroid lesions. Endocr Pathol. 2005; 16:285–293.

2. Cibas ES, Ali SZ. NCI Thyroid FNA State of the Science Conference. The bethesda system for reporting thyroid cytopathology. Am J Clin Pathol. 2009; 132:658–665.
3. Duek SD, Goldenberg D, Linn S, Krausz MM, Hershko DD. The role of fine-needle aspiration and intraoperative frozen section in the surgical management of solitary thyroid nodules. Surg Today. 2002; 32:857–861.
4. Kahmke R, Lee WT, Puscas L, Scher RL, Shealy MJ, Burch WM, et al. Utility of intraoperative frozen sections during thyroid surgery. Int J Otolaryngol. 2013; 2013:496138.
5. Gibb GK, Pasieka JL. Assessing the need for frozen sections: still a valuable tool in thyroid surgery. Surgery. 1995; 118:1005–1009.
6. Peng Y, Wang HH. A meta-analysis of comparing fine-needle aspiration and frozen section for evaluating thyroid nodules. Diagn Cytopathol. 2008; 36:916–920.
7. Wong CK, Wheeler MH. Thyroid nodules: rational management. World J Surg. 2000; 24:934–941.
8. Chang HY, Lin JD, Chen JF, Huang BY, Hsueh C, Jeng LB, et al. Correlation of fine needle aspiration cytology and frozen section biopsies in the diagnosis of thyroid nodules. J Clin Pathol. 1997; 50:1005–1009.
9. Lee YD, Cho HJ. The role of fine-needle aspiration cytology and frozen section in the operative management of thyroid nodule. Korean J Endocr Surg. 2001; 1:78–83.
10. Kesmodel SB, Terhune KP, Canter RJ, Mandel SJ, LiVolsi VA, Baloch ZW, et al. The diagnostic dilemma of follicular variant of papillary thyroid carcinoma. Surgery. 2003; 134:1005–1012.
11. McHenry CR, Thomas SR, Slusarczyk SJ, Khiyami A. Follicular or Hürthle cell neoplasm of the thyroid: can clinical factors be used to predict carcinoma and determine extent of thyroidectomy? Surgery. 1999; 126:798–802.
12. Chen H, Nicol TL, Udelsman R. Follicular lesions of the thyroid. Does frozen section evaluation alter operative management? Ann Surg. 1995; 222:101–106.
13. Boyd LA, Earnhardt RC, Dunn JT, Frierson HF, Hanks JB. Preoperative evaluation and predictive value of fine-needle aspiration and frozen section of thyroid nodules. J Am Coll Surg. 1998; 187:494–502.
14. Agcaoglu O, Aksakal N, Ozcinar B, Sarici IS, Ercan G, Kucukyilmaz M, et al. Factors that affect the false-negative outcomes of fine-needle aspiration biopsy in thyroid nodules. Int J Endocrinol. 2013; 2013:126084.
15. Siddiqui MA, Griffith KA, Michael CW, Pu RT. Nodule heterogeneity as shown by size differences between the targeted nodule and the tumor in thyroidectomy specimen: a cause for a false-negative diagnosis of papillary thyroid carcinoma on fine-needle aspiration. Cancer. 2008; 114:27–33.
16. McCoy KL, Jabbour N, Ogilvie JB, Ohori NP, Carty SE, Yim JH. The incidence of cancer and rate of false-negative cytology in thyroid nodules greater than or equal to 4 cm in size. Surgery. 2007; 142:837–844.
17. Degirmenci B, Haktanir A, Albayrak R, Acar M, Sahin DA, Sahin O, et al. Sonographically guided fine-needle biopsy of thyroid nodules: the effects of nodule characteristics, sampling technique, and needle size on the adequacy of cytologicalmaterial. Clin Radiol. 2007; 62:798–803.
18. Yoon JH, Kwak JY, Moon HJ, Kim MJ, Kim EK. The diagnostic accuracy of ultrasound-guided fine-needle aspiration biopsy and the sonographic differences between benign and malignant thyroid nodules 3 cm or larger. Thyroid. 2011; 21:993–1000.
19. Cappelli C, Castellano M, Pirola I, Cumetti D, Agosti B, Gandossi E, et al. The predictive value of ultrasound findings in the management of thyroid nodules. QJM. 2007; 100:29–35.
20. Frates MC, Benson CB, Doubilet PM, Kunreuther E, Contreras M, Cibas ES, et al. Prevalence and distribution of carcinoma in patients with solitary and multiple thyroid nodules on sonography. J Clin Endocrinol Metab. 2006; 91:3411–3417.
21. Papini E, Guglielmi R, Bianchini A, Crescenzi A, Taccogna S, Nardi F, et al. Risk of malignancy in nonpalpable thyroid nodules: predictive value of ultrasound and color-Doppler features. J Clin Endocrinol Metab. 2002; 87:1941–1946.
 XML Download
XML Download