

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Critical illness is accompanied by a hypermetabolic state related to the activation of various catabolic hormones. This situation results in elevated energy expenditure (EE), increasing the risk of malnutrition among patients [12]. In this context, accurate determination of the patients' energy requirements is of great importance, as nutrition support including optimal energy supply, is a key component for a positive clinical outcome [3].
Underfeeding has been shown to result in an increased hospital length of stay, increased incidence of complications such as infections and organ failure, and increased risk of mortality [45]. Overfeeding has also been associated with various complications, including hyperglycemia, hypertriglycemia, hepatic steatosis, azotemia, and hypercapnia, and increased rate of mortality among patients [67]. However, there remains no clear consensus among researchers, about the optimal caloric goal for the best results during nutrition support for critically ill patients, as conflicting results have been reported in the recent studies [8].
Indirect calorimetry (IC) is the gold standard for assessing energy requirements in critically ill patients [9]. However, due to the difficulty of applying IC method to certain patient conditions, its high cost and expertise requirement [9], predictive equations are commonly used to estimate the resting energy expenditure (REE). These formulas include those that have been developed using the data from healthy subjects, and others derived from critically ill patients' data. Some of the equations commonly used in critically ill patients include the Harris-Benedict (HB), Mifflin, Swinamer, Ireton-Jones and Penn State equations, and the American College of Chest Physicians (ACCP) recommendation. The aim of this study is to review the literature on energy requirements as well as assessment methods in critically ill patients.
Go to : 
STRESS RESPONSE AND ENERGY METABOLISM IN CRITICAL ILLNESS
What is stress response?
The term stress was first used in the medical literature by Sir William Osler to express the physical problems he encountered in some overworked Jews [110]. In the fields of physiology and neuroendocrinology, stress refers to those forces or factors that cause disequilibrium to an organism, threatening homeostasis [11]. Stress response has been defined as the body's nonspecific response to a variety of stressors, such as infection, fractures, surgery, burns, and wounds [12]. During stress, the priority is given to those metabolic processes that are of immediate importance in sustaining the patient's life, delaying those that are of less immediate consequence such as growth, reproduction and long-term immunity [12]. This process can result in deleterious consequences such as organ dysfunction and failure [10].
Ebb and flow phases of the stress response
David Cuthbertson first described the metabolic changes that occur in patients after a major trauma [1314]. He observed a dramatic loss of various intracellular constituents, including nitrogen (as urea), potassium, phosphorus, sulfur, and creatine under traumatic stress. He linked this loss to the systemic breakdown of lean tissue, that was later confirmed by subsequent studies, in which metabolic measurements showed a simultaneous rise in oxygen consumption at the peak of tissue breakdown in subjects [11].
The different phases of post-traumatic metabolic changes described by Cuthbertson [1314] include the ebb and flow phases. According to his observations, the short ebb phase which starts immediately after a traumatic shock, is characterized by a decrease in metabolic rate. During this phase, there is decline in oxygen consumption and body temperature, and a reduced enzymatic activity [15]. The next phase is the flow phase, which is marked by an increased catabolism, with a high oxygen consumption and an elevated EE rate. This high rate of tissue catabolism leads to a negative nitrogen balance, which is related to the rise in the rates of proteolysis, amino acid oxidation and gluconeogenesis. The flow phase is of more clinical relevance, as it lasts longer compared to the short ebb phase [16]. Complications from this catabolic state may include hyperglycemia and insulin resistance [1718]. In Cuthbertson's studies [131419], the flow phase started after 3 to 10 days and lasted until patients began the healing with metabolism returning to the anabolic state.
Hormonal and metabolic changes in response to stress
During the stress response, there is an activation of the hormones responsible for the “flight or fight” response. These hormones include glucagon, cortisol and catecholamines (epinephrine and norepinephrine) which are all catabolic hormones [12]. Their activation allows the body to quickly catabolize macronutrients from their stores, in order to cover the immediate high energy demands. For example, glucagon increases the production of glucose, mainly through the stimulation of hepatic glycogenolysis. Cortisol increases both gluconeogenesis and free fatty acid mobilization, and decreases overall protein synthesis with an increased catabolism of skeletal muscle [20]. Catecholamines increase the metabolic rate, stimulate glycogenolysis in liver and muscle as well as gluconeogenesis, and release fatty acids from adipose tissue. In addition, they stimulate the secretion of glucagon from pancreas [12].
Stress hyperglycemia commonly occurs among critically ill patients, and results from the combined effect of the above hormones which increase the hepatic glucose output through glycogenolysis and gluconeogenesis [1821]. Another contributing factor is insulin resistance which is commonly observed in critically ill patients, but stress hyperglycemia is mainly due to an increase in hepatic glucose output rather than a decrease in glucose uptake by tissues [22]. In critically ill patients, mild to moderate stress hyperglycemia and insulin resistance play a protective role, and this seems to have evolutionary roots to ensure survival [1823].
Effect of stress response on the patient's REE
The metabolic changes from the stress response have an impact on the nutritional requirements of critically ill patients, due to the higher REE in comparison to normal subjects [12]. A study [24] compared the resting metabolic rates (RMRs) of 20 men in congestive heart failure with those obtained from 40 healthy men. The measured RMR was found to be 18% higher in patients with heart failure than in controls (1,828 ± 275 kcal/day compared to 1,543 ± 219 kcal/day; p < 0.01). In another study [25], the REEs measured in 14 stable outpatients with severe chronic obstructive pulmonary disease (COPD) was compared with those measured from 7 healthy controls. The findings showed that subjects with COPD had increased REE adjusted for fat-free mass (FFM) (p < 0.001). Similar findings were observed during the work conducted by Sammarco et al. [26], in which the REE adjusted for FFM was significantly higher in patients with Crohn's disease compared to healthy controls. Monk et al. [27] measured REE in 10 critically injured patients, and their REE rose up to 55% above predicted values.
Go to :
OPTIMAL CALORIC GOAL IN CRITICALLY ILL PATIENTS
During critical illness, adequate nutritional support is an important impact on the patient's clinical outcome [3]. Both energy underfeeding and overfeeding have been associated with negative outcomes in critically ill patients [4628]. An observational study conducted by Faisy et al. [4], demonstrated that the large negative energy balance is an independent determinant of intensive care unit (ICU) mortality in very sick medical patients requiring prolonged acute mechanical ventilation, especially when energy deficit exceeded 5,021 kJ per day. In another study by Wang et al. [28] which involved ICU patients, the authors observed that energy supply less than 65% of the estimated energy requirement was associated with an increased mortality rate after adjusting for potential confounders. Weijs et al. [6] observed that in non-septic critically ill patients, early energy overfeeding (defined as an energy intake of more than 110% of measured EE) was associated with higher mortality (odds ratio [OR], 1.62; 95% confidence interval [CI], 1.07–2.44; p = 0.022).
However, the optimal caloric goal for critically ill patients remains a subject of hot debate [8]. Some studies [29303132] reported that the achievement of target energy requirements produces good outcomes, while others [33343536] reported better outcomes in patients who received lower energy than the measured or calculated caloric requirements.
Taylor et al. [29] and Martin et al. [30] observed that patients who received a greater volume of enteral nutrition (EN) had better clinical results than those who received lower volume. These findings are in agreement with the results from the work of van Schijndel et al. [31] who conducted a prospective observational cohort study including 243 medical-surgical patients. They assessed the effects of achieving optimal nutrition in ICU patients during the mechanical ventilation on mortality, and observed that female patients who reached their nutritional goals (based on the result of IC measurement) had better outcomes compared to those who did not. On the contrary, the beneficial effect of optimal feeding was not observed in male patients. In another study by Singer et al. [32] who conducted a review and analysis of literature related to nutrition in the ICU. Targeting the energy goal defined by IC is recommended for optimal energy supply in critically ill patients.
Contrary to the findings mentioned in above studies, other researchers have found that providing lower calories than the measured requirements was associated with beneficial effects. A cohort study conducted by Zusman et al. [33] evaluated the clinical outcome according to the caloric administration rate (percent of administered calories divided by measured REE [% AdCal/REE]) in ICU patients: the mortality was lower in patients with at 70% AdCal/REE in comparison to those achieving a 100% AdCal/REE. In a randomized controlled study, Arabi et al. [34], examined the effect of permissive underfeeding compared with that of target feeding (caloric goal: 60%–70% compared with 90%–100% of the calculated requirement, respectively) on the outcomes of critically ill patients. Hospital mortality was lower in the permissive underfeeding group than in the target group (30.0% vs. 42.5%; relative risk, 0.71; 95% CI, 0.50–0.99; p = 0.04). Rice et al. [35] evaluated the benefits of initial lower-volume trophic enteral feeding in comparison to initial full enteral feeding in patients with acute lung injury: compared with full enteral feeding, initial trophic enteral feeding for up to 6 days did not improve ventilator-free days, 60-day mortality, or infectious complications, but it was associated with less gastrointestinal intolerance. Similar results were reported by Rice et al. [36] who compared the initial trophic EN with full-energy EN in mechanically ventilated patients. In this study, the 2 approaches resulted in similar clinical outcomes (including ventilator-free days, ICU-free days and mortality to hospital discharge), but initial trophic EN resulted in fewer episodes of gastrointestinal intolerance.
The optimal energy target in critically ill patients remains an unsettled issue among researchers, and more studies are needed before a clear consensus can be reached. According to the recent guidelines published in 2016 by the Society of Critical Care Medicine (SCCM) and American Society of Parenteral and Enteral Nutrition (ASPEN) [9], the optimal caloric goal in critically ill adult patients was recommended as energy requirements calculated through simplistic formulas (25–30 kcal/kg/day), or published predictive equations, as well as measured by IC. The guidelines indicate IC as a method to be used for the assessment of energy requirements in critically ill patients, whenever applicable.
Go to :
ASSESSMENT METHODS FOR ENERGY REQUIREMENTS IN CRITICALLY ILLNESS
IC
IC is the gold standard for the measurement of EE in critically ill patients, and it remains as the best method whenever practical [937]. The method has served as a reference both in the development of various equations used to predict the REE in critically ill patients [3839] and in validation studies for the developed equations [404142]. The principle of IC is based on the measurement of inspired oxygen (VO2) and expired carbon dioxide (VCO2). Obtained values are used to calculate the REE by using the Weir's equation [43]. The abbreviated version of this equation is commonly used, and it is as follow [44]:
REE (kcal/day) = (3.941 × VO2 [L/min] + 1.106 × VCO2 [L/min]) × 1,440
where VO2 is the volume of consumed O2 and VCO2 is the volume of produced CO2.
In many instances, IC method may be limited by the high cost of machines and the lack of qualified staff. In critically ill patients, other factors that may limit the use of IC include the presence of air leaks or chest tubes, supplemental oxygen (e.g., nasal cannula, bilevel positive airway pressure), ventilator settings (fractional inspiratory oxygen and positive end-expiratory pressure), continuous renal replacement therapy (CRRT), anesthesia, physical therapy, and excessive movement [945].
Predictive equations for REE in critically ill patients
Various equations have been in use for the prediction of REE in critically ill patients, especially as the measurement by IC is not always practical. In this paper, we discussed some of REE equations which are commonly used in critically ill patients (Table 1) and which have been validated among the critically ill patients (Table 2).
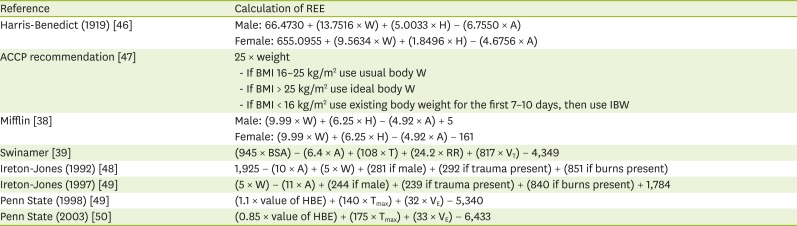
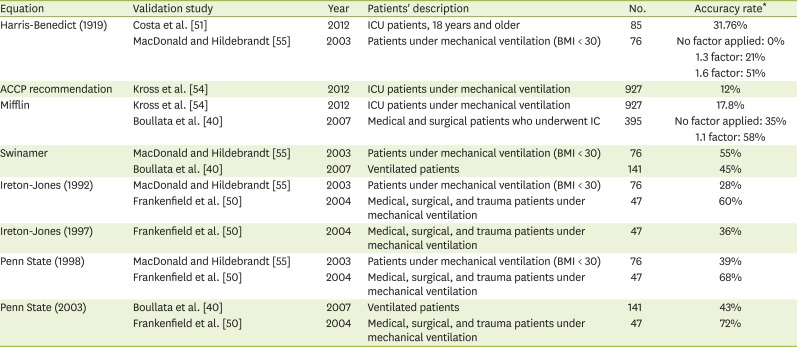
Table 1
Equations for predicting REE (kcal/day)
| Reference | Calculation of REE |
|---|---|
| Harris-Benedict (1919) [46] | Male: 66.4730 + (13.7516 × W) + (5.0033 × H) − (6.7550 × A) |
| Female: 655.0955 + (9.5634 × W) + (1.8496 × H) − (4.6756 × A) | |
| ACCP recommendation [47] | 25 × weight |
| - If BMI 16–25 kg/m2 use usual body W | |
| - If BMI > 25 kg/m2 use ideal body W | |
| - If BMI < 16 kg/m2 use existing body weight for the first 7–10 days, then use IBW | |
| Mifflin [38] | Male: (9.99 × W) + (6.25 × H) − (4.92 × A) + 5 |
| Female: (9.99 × W) + (6.25 × H) − (4.92 × A) − 161 | |
| Swinamer [39] | (945 × BSA) − (6.4 × A) + (108 × T) + (24.2 × RR) + (817 × VT) − 4,349 |
| Ireton-Jones (1992) [48] | 1,925 − (10 × A) + (5 × W) + (281 if male) + (292 if trauma present) + (851 if burns present) |
| Ireton-Jones (1997) [49] | (5 × W) − (11 × A) + (244 if male) + (239 if trauma present) + (840 if burns present) + 1,784 |
| Penn State (1998) [49] | (1.1 × value of HBE) + (140 × Tmax) + (32 × VE) − 5,340 |
| Penn State (2003) [50] | (0.85 × value of HBE) + (175 × Tmax) + (33 × VE) − 6,433 |
REE, resting energy expenditure; W, weight (kg); H, height (cm); A, age (years); ACCP, American College of Chest Physicians; BMI, body mass index (kg/m2); IBW, ideal body weight (kg); BSA, body surface area (m2); T, body temperature (°C); RR, respiratory rate (breaths/min); VT, tidal volume (L); HBE, Harris-Benedict equation; Tmax, Maximum body temperature in the past 24 hour (°C); VE, minute volume (L/min).
![]()
Table 2
Accuracy rates for REE predictive equations
| Equation | Validation study | Year | Patients' description | No. | Accuracy rate* |
|---|---|---|---|---|---|
| Harris-Benedict (1919) | Costa et al. [51] | 2012 | ICU patients, 18 years and older | 85 | 31.76% |
| MacDonald and Hildebrandt [55] | 2003 | Patients under mechanical ventilation (BMI < 30) | 76 | No factor applied: 0% | |
| 1.3 factor: 21% | |||||
| 1.6 factor: 51% | |||||
| ACCP recommendation | Kross et al. [54] | 2012 | ICU patients under mechanical ventilation | 927 | 12% |
| Mifflin | Kross et al. [54] | 2012 | ICU patients under mechanical ventilation | 927 | 17.8% |
| Boullata et al. [40] | 2007 | Medical and surgical patients who underwent IC | 395 | No factor applied: 35% | |
| 1.1 factor: 58% | |||||
| Swinamer | MacDonald and Hildebrandt [55] | 2003 | Patients under mechanical ventilation (BMI < 30) | 76 | 55% |
| Boullata et al. [40] | 2007 | Ventilated patients | 141 | 45% | |
| Ireton-Jones (1992) | MacDonald and Hildebrandt [55] | 2003 | Patients under mechanical ventilation (BMI < 30) | 76 | 28% |
| Frankenfield et al. [50] | 2004 | Medical, surgical, and trauma patients under mechanical ventilation | 47 | 60% | |
| Ireton-Jones (1997) | Frankenfield et al. [50] | 2004 | Medical, surgical, and trauma patients under mechanical ventilation | 47 | 36% |
| Penn State (1998) | MacDonald and Hildebrandt [55] | 2003 | Patients under mechanical ventilation (BMI < 30) | 76 | 39% |
| Frankenfield et al. [50] | 2004 | Medical, surgical, and trauma patients under mechanical ventilation | 47 | 68% | |
| Penn State (2003) | Boullata et al. [40] | 2007 | Ventilated patients | 141 | 43% |
| Frankenfield et al. [50] | 2004 | Medical, surgical, and trauma patients under mechanical ventilation | 47 | 72% |
REE, resting energy expenditure; ICU, intensive care unit; BMI, body mass index; ACCP, American College of Chest Physicians; IC, indirect calorimetry.
*Accuracy rate: percentage of subjects having the REE predicted within 10% of the measured value.
![]()
HB equation (1919)
One of the well-known REE equations and commonly used in critically ill patients, is the HB equation [46] which was developed in 1919 using data from healthy participants, including 136 men, 103 women and 94 new-born infants. However, many studies reported that applying HB equation to critically ill patients is inaccurate [4142515253]. For example, Costa et al. [51] compared the REE predicted by HB equation with the measurements by IC in 85 hospitalized critically ill patients. The equation was found to be accurate only in 31.76% of the subjects. A work by Koukiasa et al. [52] demonstrated that HB equation underestimated energy requirements, in 30 non-septic critically ill patients with spontaneous intracranial hemorrhage (SICH). In addition, they observed that the equation was inefficient in detecting individual variability of REE in the participants. The HB equation was also assessed by Martins et al. [53], in 30 critically ill surgical patients under mechanical ventilation. In this study, a low correlation was observed between measured and predicted REE, with the Spearman's r of only 0.57. Picolo et al. [42] compared the REE measured by IC with REE calculated by using the HB equation, in 205 critically ill patients undergoing mechanical ventilation. The findings showed that the HB equation was inaccurate and cannot be substituted for IC in critically ill patients.
ACCP recommendation
The ACCP recommendation was published in the 1997 consensus statement [47], providing guidelines on the nutrition management of ICU patients. Concerning the energy supply to patients, the guideline recommends 25 kcal/kg of usual body weight for most patients. In case of obese patients (body mass index [BMI] ≥ 25 kg/m2), the recommendation is to estimate energy requirements based on the ideal body weight. In patients whose BMI < 16 kg/m2, it is recommended to calculate energy requirements based on the patient's current body weight during the first 7–10 days, then the estimation should be based on the ideal body weight [4047]. In 2 validation studies, this equation has been found to yield inaccurate results in critically ill patients, with the accuracy rate of 12% [54] and the coefficient of determination (R2) value of only 0.24 [41].
Mifflin equation
The Mifflin equation [38] was developed based on the data from 498 healthy subjects, including 251 men and 247 women. Validation studies of this equation have reported that the equation was inaccurate in critically ill patients [4054]. Boullata et al. [40] evaluated the accuracy of 7 REE predictive equations including the Mifflin equation in 395 hospital patients, and reported that all the equations resulted in clinically unacceptable errors. The Mifflin equation gave only 35% of accurate predictions. When the factor of 1.1 was applied, the rate of accurate predictions was 58%.
Swinamer equation
The Swinamer equation was developed based on data from 112 mechanically ventilated, critically ill patients. This equation was determined from variables that contributed greater than 3% to the variance of EE, namely the body surface area, age, respiratory rate, tidal volume, and body temperature [39]. The use of this equation has been limited by the difficulty to obtain the information on all contributing variables, that is, only 2 validation studies have been conducted so far [4055]. In the work of MacDonald and Hildebrandt [55], they retrospectively assessed the Swinamer equation in 76 ICU patients, and found the accuracy rate to be 55%. In another study, Boullata et al. [40] evaluated the accuracy of this equation in 141 ventilated patients, and they found the accuracy rate was 45%.
Ireton-Jones equations (1992 and 1997))
This equation is one of the most commonly used in ventilated patients. It was first developed in 1992 [48], using the data from 200 patients with mean age of 43 years. The validation study by MacDonald and Hildebrandt [55] reported that an accuracy rate of the equation was 28%, while another work by Frankenfield et al. [50] demonstrated the accuracy rate of the equation was 60%. In 1997, Ireton-Jones and Jones [49] developed a new equation for ventilated patients, by re-analyzing the data that had been used to derive the previous equation with the objective of improving its accuracy. The revised equation resulted in an improved accuracy rate of 58%. However, a validation study conducted by Frankenfield et al. [50], reported this equation to be accurate in only 36% of subjects.
Penn State equations (1998 and 2003)
The original Penn State equation was published in 1998 [49]. It was developed based on data from 169 mechanically ventilated surgery and medicine patients. In this equation, the adjusted body weight was used in case of obese patients. Validation studies for this equation reported the accuracy rates of 68% [50] and 39% [55]. In 2003, the Penn State equation was modified [50]. Instead of the adjusted body used in the previous equation, the new equation used the actual body weight in obese subjects. In 2 validation studies, accuracy rates were 43% [40] and 72% [50] of the subjects, respectively.
Go to :
CONCLUSION
Critically ill patients commonly have higher REE than healthy individuals. It may indicate that ciritical ill patinets haveincreased energy requirements. To ensure adequate nutritional support to the critically ill patients, it is important to accurately assess EE in individual patients. Compared with IC, the gold standard, the existing REE formulas are inaccurate, thereby increasing the risk of underfeeding or overfeeding. This challenge concerns not only the equations developed from the data of healthy populations, but also those that have been specifically developed in critically ill patients. Further studies are needed to develop the equations that are more accurate so as to provide optimal energy to patients. The SCCM and ASPEN guidelines recommend the caloric goal in critically ill adult patients as energy requirements calculated either through simplistic formulas (25–30 kcal/kg/day) or published predictive equations, as well as measured by IC.
Go to :
 XML Download
XML Download