

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obesity is a primary risk factor for type 2 diabetes, thus increasing the prevalence of type 2 diabetes. Additionally, a cohort study by Sasai et al. [1] revealed that in middle-aged and older Japanese subjects, obesity was associated with increased risk of type 2 diabetes. According to the results of a study conducted in the United States, obesity and diabetes are continuously increasing in both sexes and in all age groups, races, and educational levels [2].
The American Diabetes Association guidelines suggest that weight loss may decrease the risk of type 2 diabetes in prediabetic subjects [3]. Weight loss of approximately 5% in overweight or obese diabetic patients may help manage blood glucose and further reduce the need for glucose-lowering medications [3]. In an observational cohort study on overweight American adults, intentional weight loss was associated with a lower rate of the development of diabetes [4]. According to previous studies, nutrition interventions have significant effects on weight loss [567]. Weight loss by regulating lifestyle interventions, including nutrition interventions, has been associated with a lower incidence of diabetes [8].
Previous studies on subjects with high risk of diabetes have confirmed the positive effects of improved lifestyle including weight control on the incidence of type 2 diabetes [910111213]. The incidence of diabetes in subjects achieved weight loss decreased compared with a control group [910111213]. The 2015 Treatment Guidelines for Diabetes [14] published by the Korean Diabetes Association recommend that governments make efforts to prevent diabetes, but such studies have not yet been conducted in Korea. Therefore, the aims of this study were to perform continuous nutrition interventions focused on lifestyle changes, including weight loss, and to analyze intervention-related changes in subjects with prediabetes.
CASE
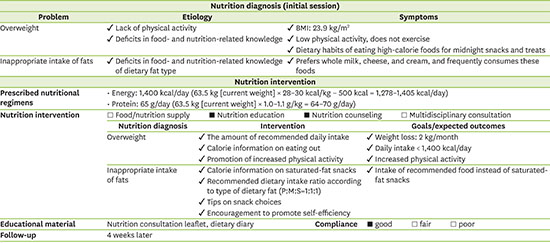
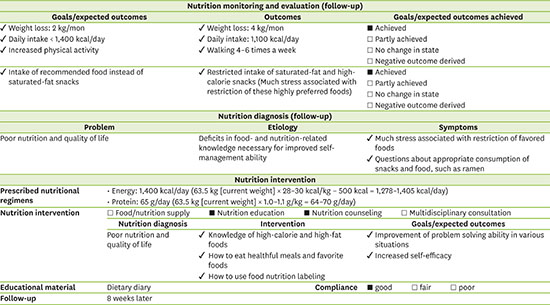
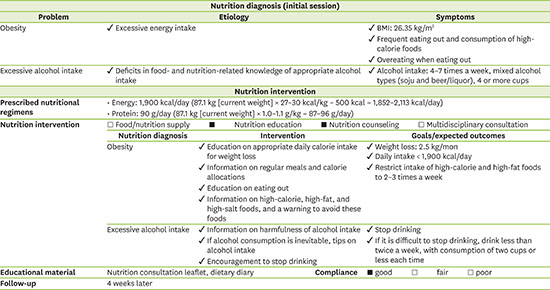
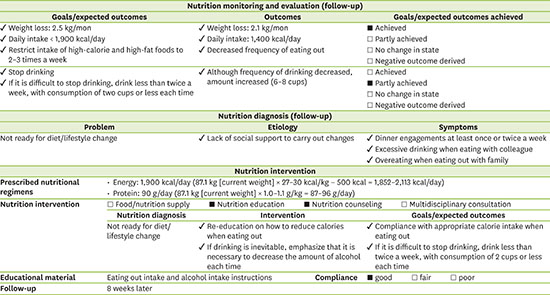
The participants of this study comprised two subjects at high-risk of type 2 diabetes. Subjects received lifestyle interventions, including a nutrition intervention, from December 2016 to July 2017.Our nutrition intervention description was presented on Figure 1. They first visited Kyung Hee University Medical Center for a National Health Insurance Corporation examination or a health examination. They were aged 30–65 years, with a body mass index (BMI) of ≥ 23 kg/m2 and had fasting blood glucose levels of 100–125 mg/dL. Each subject was personally interviewed at his or her first visit to our medical center to provide information on his or her general characteristics and lifestyle behaviors, such as smoking, alcohol drinking, exercise, and dietary intake. Information on dietary intake was obtained by a trained clinical dietitian using a 3-day record, and the data were analyzed using the Computer Aided Nutritional Analysis program, version 5.0 (Korean Nutrition Society, Seoul, Korea). Clinical characteristics of the subjects were obtained from their medical records.
Figure 1
Nutrition intervention protocol.
*Nutrition intervention was conducted according to the protocol, but the contents of nutrition education varied by the individual's dietary habit.

Case 1
1) The first visit
The first subject was a 53-year-old Korean woman who had not been diagnosed with diabetes. The subject visited the medical center at December 2016. Then subject was 163.7 cm in height and 63.5 kg in weight (BMI, 23.7 kg/m2; overweight by Asian standards). Her glycated hemoglobin (HbA1c) level was 6.1% and her fasting glucose sugar level was 104 mg/dL (Table 1).
Table 1
Clinical characteristics of the subject in each case at baseline

Three months before the visit to the medical center, the weight of the subject had increased to 68 kg because of increased intake of snacks, including late-night snacks. After that, the subject had adjusted the diet and reduced the weight by 3 kg. The subejct preferred to eat dairy products (e.g., whole milk and cream cheese), bread (e.g., red bean bread and cream bread), and snacks. At first visit, the subject was sufficiently motivated for weight management and was aware of the necessity of weight loss. Two months ago, the subject had tried to refrain from snacking and regularly ate three meals a day. The subject usually ate meals with side dishes of vegetables and fish of equal size at home. The subject's breakfast comprised cereal, fruits, tofu, and vegetables. Usual energy intake was approximately 1,400–1,500 kcal/day (Table 2). The subject engaged in a low level of physical activity, but had recently started walking. We provided information on appropriate calorie intake and identified a target weight to be achieved by the next visit. We also provided calorie information in foods the subject regularly consumed as snacks and how to choose appropriate snacks, including how to read the Nutrition Facts label when buying processed foods. We also explained the benefits of regular exercise and encouraged the subject to engage in it.
Table 2
Clinical characteristics of the subject in case 1 after nutrition counseling
2) The second visit
In January 2017, four weeks after the first visit, the body weight of the subject was 59.5 kg. This was approximately 4 kg less than the weight at the time of the first visit (Table 2). The subject had regularly consumed three meals a day over the past 4 weeks. In addition, the subject had consumed 100–150 g of vegetables and 50 g of fish and meat for every meal. The subject had not eaten any snacks or sweet bread, and the subject drank a cup of black coffee or low-fat latte a day. The subject walked for exercise about 1 hour a day for more than 4 days a week. The subject was proud of the weight loss that she had achieved over the 4 weeks with a steady diet and exercise and demonstrated a commitment to maintaining improved eating habits in the future. We affirmed the weight loss success and explained that it was very important to ensure that the weight did not increase again. We also encouraged the subject to maintain her improved eating and exercise habits.
3) The third visit
In March 2017, the subject made third time visit to our medical center. The weight was 57.7 kg, which was 5.8 kg less than the weight at the time of the first visit (Table 2). The subject had tried to maintain a balanced diet in every meal and to maintain the weight loss. However, since February, the subject had had frequent meetings and her consumption of high-calorie and high-fat foods (e.g., pork belly, gimbap, and tteok-bokki) had become more frequent. The subject had been eating snacks such as bread, corn, chocolate, and jelly more frequently than at the time of the last visit. However, on the days that the subject ate out or engaged in overeating, the subject walked from 20,000 to 30,000 steps more than 4 times a week. We provided an information on the challenge of calorie consumption and strategies on appropriate eating when eating out.
4) The fourth visit
In June 2017, the subject's weight was 57 kg, which was 6.5 kg less than the weight at the time of the first visit (Table 2). Over the past 6 months, the subject had managed to lose approximately 10% of the initial weight. However, the subject had not been able to consistently manage the diet over the past 3 months. Dietary diary analysis showed that the average calorie intake was approximately 1,700 kcal (Table 2). In particular, over the past 3 months the subject had often eaten out. When eating out, the subject often ate high-calorie foods such as pasta, pizza, and hamburgers. Despite of increasing calorie intake, the subject had been frequently exercising, such as walking and cycling. We encouraged the success in achieving a weight loss of 10% over 6 months and commended the subject to maintain the healthy eating and regular exercise.
Case 2
1) The first visit
The second subject was a 46-year-old Korean man who had not been diagnosed with diabetes. The subject visited our medical center in January 2017. The subject was 181.7 cm in height and 87.1 kg in weight (BMI, 26.4 kg/m2). The HbA1c level was 5.7% and the fasting glucose sugar level was 107 mg/dL (Table 1).
The subject had a high standard of education and was interested in weight loss, and as such, the subject had tried various diets in the past, but had never been successful in losing weight. At the time of first visit, the subject recognized the necessity of weight control, but did not translatethe recognition into obvious action. The subject usually had frequent company meetings, and often ate meat or raw fish when eating out. The subject drank alcohol more than 4 times a week and drank a variety of drinks, including soju, whiskey, liquor, and beer. The subject drank more than 4 cups of alcohol each time. Over the past 3 days, the subject had consumed only yogurt and vegetable juice for weight control. The subject engaged in a low level of physical activity, but had recently started doing core exercises for 30 minutes a day at home. We provided information on appropriate calorie intake and identified a target weight to be achieved by the next visit. We also provided calorie information of alcoholic drinks and foods often consumed and explained how to make appropriate menu choices when eating out. In addition, we explained the benefits of limiting alcohol intake and encouraged the subject to stop drinking.
2) The second visit
In February 2017, 4 weeks after the first visit, the weight of the subject was 85.0 kg, which was approximately 2 kg less than the weight at the time of the first visit (Table 3). The subject ate lunch and dinner outside, usually eating a lunch box or a one-dish meal at a cafeteria. The subject had tried to reduce the amount of rice he consumed. The subject still had many dinner engagements for work, but the frequency of the alcohol consumption had decreased to once a week. However, the amount of alcohol consumed each time had increased from four glasses of soju and beer to eight glasses when the subject had a meat as a main dish. For snacks, the subject had been having a latte and a small amount of nuts. The physical activity had increased; the subject walked a lot on days that he overate and had maintained thecore exercises at home. Still the subject had ate out many times since last visit to the center, and the subject was stressed whenever he ate out. The subject still had a lot of interest in weight loss, but the actual willingness to act seemed to be weaker. The subject also showed a lot of interest in nutritional counseling. We again gave him a calorie information of the foods often consumed when eating out, how to make appropriate menu choices, and how to reduce calorie intake upon eating out. We reiterated the appropriate amount of drinking and encouraged the subject to stop drinking. In addition, we encouraged the subject to continue walking and the core exercises.
Table 3
Clinical characteristics of the subject in case 2 after nutrition counseling
3) The third visit
In March 2017, the subject's weight was 82.9 kg, which was 4.2 kg less than the weight at the time of the first visit (Table 3). The subject had tried to eat regularly, and the subject's calorie intake was lower than that of the second visit. When the subject was too busy to eat breakfast, the subject consumed a bread with coffee. The amount and frequency of snacking had greatly reduced. However, as the subject's work became busy, the subject was not able to exercise as much as he had before. We affirmed the weight loss of the subject and encouraged the subject to ensure that the weight had not increased again.
4) The fourth visit
The subject visited our medical center for the fourth time in July 2017. The weight was 84.9 kg, which was 2.2 kg less than the weight at the time of the first visit (Table 3). The subject had finally managed to lose 2.5% of thr weight at the time of the first visit over the course of 6 months. Since the last month before this visit, the subject had had many dinner engagements with friends and colleagues and had eaten more high-calorie foods such as high-fat meats and stews. In addition, the frequency and amount of the alcohol consumption had significantly increased since the time of the last visit. Dietary diary analysis showed that the subject's average calorie intake was approximately 2,100 kcal, and the proportion of fat was 43%. Both the calorie and fat intake rates were higher than those at the time of the last visit (Table 3). Also, it is important to note was that the subject's calorie intake did not reflect the alcohol intake. In an interview, we estimated the calorie intake from each time the subject consumed alcohol to be approximately 1,100 kcal. The intake of high-fat foods and overconsumption of alcohol were due to the subject's frequent dinner appointments, which had been a problem since the time of the subject's first visit. This had not been improved significantly. Moreover, the subject had ceased exercising. We analyzed obstacles to address these problems and set goals that could be implemented to overcome these obstacles. In addition, we provided the subject an information on ingestion tips to maintain progress of these goals.
DISCUSSION
In both cases, at the time of their last visit, the subjects had increased their calorie intake compared with that of their first visit, but had successfully decreased their body weight. In case 1, the subject's calorie intake was the highest at the time of the last visit (Table 2). However, the subject had begun to increase the physical activity on days when the subject ate a meal outside or a lot of snacks, and the subject had begun to reduce her meal or snack intake the following day. In conclusion, overall eating habits of the subject had become healthier in case 1. It is thought that the continuous counseling and monitoring given to the subject improved the subject's self-management ability of the eating habits. In addition, as the intervention proceeded, the subject's carbohydrate intake decreased and the protein intake increased. This is thought to be the result of efforts to reduce the consumption of snacks such as confectionery and bread and to consume foods rich in protein such as meat, fish, and tofu for every meal. In addition, the feelings of bond and trust between the clinical team and the subjects became tighter with the counseling conducted at regular intervals and facilitated maintaining weight loss through improved self-efficacy and self-management ability. In fact, several studies suggested that nutrition intervention have significant beneficial effects on weight loss [567]. A study by Appel et al. [15] revealed that an in-person intervention had a significant positive effect on weight loss in obese American subjects compared with a control condition.
In case 2, the subject's calorie intake and fat ratio had increased over the course of the 4 counseling sessions (the ratio of carbohydrate:protein:fat was at the 1st visit, 61:13:26; 2nd visit, 52:16:32; 3rd visit, 54:12:34; and 4th visit, 41:16:43) (Table 3). Due to the demographic characteristics of office workers, it is assumed that he frequently attended company dinners, ate outside, and eating high-fat meat on those occasions.
In the subject of case 2, the amount of the alcohol consumption was not reflected in subject's dietary diary analysis, despite of more than approximately 1,000 kcal from alcohol intake each time. The subject did not make significant progress on reducing his drinking, which was the primary problem. It can be assumed that the lack of practice and will, as well as social and environmental factors, did not support a positive change in this respect.
Thus, we taught both subjects how to consume good-quality fat rather than poor-quality fat, how to make appropriate menu choices when eating out, how to moderate alcohol consumption, and so on. We also provided nutritional counseling that focused on how to increase physical activity and improve self-regulation after overeating, which could contribute to improved self-management ability. In addition, social and environmental conditions related to food cultures are important to improve eating habits; therefore, it is considered that social support is necessary for successful behavioral change.
In conclusion, as a result of conducting a total of four nutrition education and counseling sessions over a 6-month period, it seems that education and personalized, in-depth intervention had a positive influence on both subjects' weight loss. It is evident that the expert knowledge of the clinical dietitian, the provision of patient-centered education based on coping ability in various situations, and quality of the relationship and degree of trust between the patient and clinical dietitian are important to encourage continuous practice.
Many studies have suggested that diabetes self-management education (DSME) provides the foundation to support individuals for improving their quality of life and forming healthy eating habits [16171819]. However, as a social DSME programs has not yet designed for Koreans, it is necessary to develop and implement such programs.
In addition, as self-management is continuously performed in day-to-day life, this should be cared by specific system based on social support and not only by a single educational session delivering how to manage a chronic disease. Continuing education and a more professional andsystematic clinical team that comprises doctors, clinical dietitians, and nurses need to be well-established for implementing of DSME program for Korean with diabetes and prediabetes.
 XML Download
XML Download