

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Inflammatory bowel disease (IBD) is a chronic idiopathic inflammatory disease that is represented by ulcerative colitis and Crohn's disease. IBD is caused by a combination of genetic and environmental factors and the patients suffer from nausea, vomiting, loss of appetite, headaches, and diarrhea during treatment [1]. Moreover, it is reported that maintaining a good working status or daily life is difficult for the patients because of repeated relapse of their works. Such situation can lead anxiety, depression, or feeling of socially isolated in patients and compromise their quality of life [23]. The incidence of IBD due to dietary factors has increased specifically in patients with an increase in fat and protein intake and the lack of fruits and vegetables intake from the diet [4]. Studies have shown that when high levels of linoleic acid are consumed, a high intake of red and processed meat increases the risk of developing ulcerative colitis as well as relapse. The association between food intake patterns and changes in intestinal bacteria has been emphasized in several studies [567]. Ulcerative colitis and Crohn's disease are associated with a 20%–75% loss of body weight and electrolyte imbalance [8]. Various factors are involved in causing nutritional deficiencies in individuals with IBD, including decreased oral intakes, metabolic disorders, increased nutritional requirements, drug interactions, and malabsorption [9]. In addition, nutritional disorders can occur due to prolonged periods and indiscriminate manner of food restriction for reducing discomfort from IBD symptoms.
Thus, nutrition goals for patients with IBD need to be coordinated so that patients can better manage themselves with the aim of maintaining or improving a balanced nutritional status through appropriate provision of nutrients according to their treatment conditions [10]. However, nutrition studies conducted for Korean patients with IBD are very rare. This study was performed to assess the nutritional status of patients with IBD and to analyze whether the diet or nutritional imbalance varies depending on food restriction. Our findings will serve basic data to future clinical nutrition research for IBD patients.
MATERIALS AND METHODS
Study subjects
The study subjects were patients with confirmed IBD who visited the digestive division of Soonchunhyang University Hospital in Gyeonggi-do. The first 112 patients participated but only the final 104 results were used for the study; results from 8 patients were excluded due to denial or missing data. The participants were fully informed of the purpose, need, and method of this study and asked for their consent. The research design and protocol were approved by Institutional Review Board of Soonchunhyang University (approval number: 2015-BM-002-01). Based on the study purpose, the subjects were classified into 2 groups (food exclusion group, n = 49; food non-exclusion group, n = 55) through interviews with a clinical dietitian.
Variable measurements and definitions
Subjects' body mass index (BMI) was calculated using height and weight. We obtained data about the disease diagnosis period (< 1, 1–3, ≥ 3 years) and IBD classification (Crohn's disease or ulcerative colitis). Disease activity reflected the medical record information as well as confirmation from the physician. The patients' nutritional status was assessed by a clinical dietitian using a subjective global assessment method and nutritional status was classified as adequate, mild or moderate malnutrition, or severe malnutrition.
After the diagnosis, beliefs and attitude related to the patients' usual diet were investigated. The questions were based on previous research journal and were reviewed by the researchers [1112]. ‘Do you think you are important to meals in the beginning and during the period of IBD diagnosis?’, ‘Do you have a dietary modification?’, ‘Do you think that diet could play a role in causing disease relapse?’, ‘Do you think you should avoid food to prevent disease relapse?’, ‘In case of relapse, what diet do you believe can improve disease symptoms?’, ‘Do you received nutrition education and management?’, ‘Do you want a nutritional education and professional management?’ Dietary habits assessed were about drinking, smoking, exercise, regularity of meals, eating speed, and frequency of eating out. In order to examine the degree of restriction of food intake, a questionnaire was analyzed for a list of foods that are usually restricted in the diet. In order to evaluate nutrient intake, 3-day food record method was conducted and the data was analyzed using the computer-aided nutritional analysis program (CAN-Pro 4.0; Korean Nutrition Society, Seoul, Korea).
Statistics analysis
Statistical processing and analysis for all data collected from the investigation were performed by using the SPSS program (ver. 18.0; SPSS Inc., Chicago, IL, USA). To identify factors differing between the groups, the independent t-test was used for continuous variables including nutrient factors and the equal-variance, χ2 test, or Fisher's exact test for categorical variables. For all analyses, p < 0.050 was considered statistically significant.
RESULTS
The characteristics of the 104 patients can be found in Table 1. The total number of subjects in the food exclusion group was 49 (47.1%) and the mean age was 39.4 years. The mean age of the food non-exclusion group was significantly lower than that of the food exclusion group (p = 0.016). The mean BMI of all subjects was 23.6 kg/m2 and the diagnosis period was < 1 year in 23.1%, 1–3 years in 36.5%, and ≥ 3 years in 40.4% of all subjects. The type of IBD was Crohn's disease in 58.7% and ulcerative colitis in 41.3%. For current disease activity 27.9% of patients were categorized as active stage and there was no significant difference between the 2 groups.
Table 1
Demographics and characteristics of the IBD patients
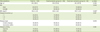
Data were reported as mean ± standard deviation or mean (standard deviation) for continuous variables and frequency (percentage) for categorical variables. p values were calculated by χ2 test.
IBD, inflammatory bowel disease; BMI, body mass index.
*p value was calculated by independent t-test.
![]()
The nutritional status was adequate for 65.4% of the patients in the food exclusion group while there was mild-moderate malnutrition in 22.4% and severe malnutrition in 12.2% of the patients. The respective rates in the food non-exclusion group were 76.4%, 18.2%, and 5.5%. The rate of malnutrition in the food exclusion group was significantly higher than the non-exclusion group (p = 0.007) (Figure 1).
 | Figure 1Comparison of nutritional status between groups. Data were reported as frequency (percentage) for categorical variables. p value for the significant difference between 2 groups is 0.007 and was calculated by χ2 test.
|
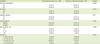
As a result of the analysis of beliefs and attitudes toward diet, the rate of dietary intervention was 77.6% in the food exclusion group and 36.4% in the food non-exclusion group, and there was a significant difference between the 2 groups (Table 2). Total of 38 patients had a dietary modification by harmful food restriction (50.0%), harmful recipes restriction (21.0%), and adjusting the amount of meals (15.8%). In addition, 73.5% of those in the food exclusion group indicated that food should be avoided in order to prevent relapse of disease, as compared to 20.0% of those in the food non-exclusion group. The percentage of people who wanted nutrition education and management was 83.7% for the food exclusion group and 67.3% in the food non-exclusion group.
Table 2
Diet beliefs and educational demand of the IBD patients

Data were calculated based on answer ‘yes.’ Data were reported as frequency (percentage) for categorical variables and p values were calculated by χ2 test.
IBD, inflammatory bowel disease.
![]()
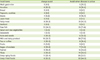
In part of the survey on eating habits and lifestyle (Table 3), there was a significant difference only in drinking and eating out between the 2 groups. Despite the fact that there was no difference in the ratio of men and women between the 2 groups, the food non-exclusion group had a high rate of alcohol consumption. The rates of regular exercise and eating regular meals was < 50%. The frequency of eating out was 1–3 times per month in the food exclusion group and 1–2 times per week in the food non-exclusion group.
Table 3
Life habit and eating behavior of the IBD patients
Data were reported as frequency (percentage) for categorical variables and p values were calculated by χ2 test.
IBD, inflammatory bowel disease.
![]()
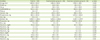
In the food exclusion group, the most frequently restricted foods were milk and dairy products, raw fish, fatty meats, noodles, and deep-spicy foods (Table 4). Milk and dairy products, raw fish, deep-spicy foods, deep-fried foods, and fatty meat were restricted in high priority when the disease was activated.
Table 4
Food items of food exclusion group (n = 49)
![]()
As a result of nutrient intake analysis, there was no significant difference in energy, protein, fat, carbohydrate, or fiber between 2 groups (Table 5). Calcium, zinc, and vitamin A intake in the food exclusion group were significantly lower than those in the food non-exclusion group.
Table 5
Nutrient intake status of the IBD patients
Data were reported as mean ± standard deviation for continuous and p value was calculated by independent t-test.
IBD, inflammatory bowel disease.
![]()
DISCUSSION
The deliberate diagnosis of ulcerative colitis and Crohn's disease is important for IBD. The ultimate goal of IBD treatment is to improve symptoms of acute episodes and to improve the quality of life and health of patients by treating patients well [13]. In recent years, the concept of remission has changed, and the empirical contents such as improvement of clinical symptom of the patient have been reflected as a new concept of ‘deep remission’ [14].
The rate of malnutrition in patients with IBD is very high and the immune system damage caused by malnutrition has been reported to have a negative effect on treatment response. In the case of Crohn's disease, nutritional support is needed as a primary treatment of disease, and comparative studies with steroid treatment have proved to be effective, but ulcerative colitis has not been recognized as an absolute necessity for primary treatment. However, there is a common opinion that secondary treatment is needed to treat malnutrition for both diseases [1516]. For patients with IBD parenteral nutrition and the guideline for tube feeding and oral intake according to intestinal function is recommended. In case of resting period, the recurrence rate is low when a normal diet is added to a basal diet [17].
Patients with IBD have high rates of iron, calcium, vitamin B12, and vitamin D deficiencies. One of the causes for malnutrition is a dietary adjustment to the patient's own experience and beliefs. The degree of dietary intolerance was similar between patients with Crohn's disease and ulcerative but studies have also identified food intolerance in artificial sweeteners, grains, dairy products, and yeast in IBD patients [1819]. Recent changes in the concept of IBD treatment are not adequate to control patients' beliefs and experiences. Still, there is a concern about an adverse effect of the diet which is based on of patients' prolonged absolute belief. Individualized adjustments are therefore necessary to accommodate the patient's disease and condition. In this study, the food exclusion group had a higher rate of Crohn's disease patients and the belief that food control decreased recurrence of symptoms compared to food non-exclusion group. However, the intake of some nutrients was poor, and the rate of malnutrition was high in patients in the food exclusion group.
This study has a limitation. In this study the patients were not classified according to disease or activity and the nutrient intake of study patients was assessed regardless of adequate intake according to individual nutritional requirement. What is interesting is that the rate of receiving nutrition education or management is very low and the rate of requests is very high. According to an international study, about half of Crohn's disease patients who had weight loss experienced pleasure of eating according to the management of specialists and reported that those changes affected the recurrence of disease symptoms [20]. There are not many domestic or foreign studies evaluating this concept between nutrition and IBD management and this is an important area for future research. It is considered that dietary factors that should be treated in high priority for the social life of IBD patients.
 XML Download
XML Download