

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Migraine is known as a chronic disease related to brain neurovascular system [1]. Migraine is estimated to be the third cause of disability, according to the Global Burden of Disease 2015, in individuals under the age of 50 [2]. Also, migraine can increase the risk of nervous disorders, such as stroke, and lead to reduce the quality of life [34].
According to the International Headache Society (IHS) criteria, migraine has 2 subtypes due: migraine with aura and without aura that this classification is associated with the presence or absence of transient disturbance in motor function, visual, language, or sensory. However, the most migraine patients have migraine without aura [56]. One of the current symptoms of the migraine is recurrent headaches that may be followed by gastrointestinal disorders, like nausea and vomiting [78]. Also, these symptoms can be affected by environmental factors, like light and noise [9].
The major mechanism about the pathophysiology of migraine is not completely clear, but studies showed that various factors, such as diet and lifestyle, may play an important role [1011]. It seems the B vitamins group as an important part of diet affects clinical symptoms of the migraine [1213].
According to previous studies, thiamine supplementation may lead to an improvement in migraine headaches in Wernicke-Korsakoff syndrome. Nausea, vomiting, and anorexia may contribute the lower intake of thiamine among migraine patients with headaches, this can describe the relation between migraine headaches and thiamine status.
Low thiamine intake leads to increased risk of the Wernicke-Korsakoff and frequent headaches [141516]. Thus, the relation between thiamine status and migraine headaches has suggested the necessity of study about dietary intake of the thiamine in migraine patients. Also, there are many studies related to the B vitamins group status and migraine headaches [1317], but the studies about thiamine are limited. Thus, the main purpose of this study is to compare the dietary intake of thiamine in migraine patients and healthy people, and its relation to the frequency of migraine attacks.
MATERIALS AND METHODS
Based on the case-control design, current study was conducted on 50 migraine patients in Isfahan, Iran, in 2017. Patients were included based on: 1) Being in the range of 20 to 60 years; 2) Interested in participating in the study; 3) Suffering migraine; and 4) Not receiving drugs for certain diseases, such as stroke, renal, and heart diseases.
Confirmation of migraine diagnosis was carried out using the IHS criteria [5] by an expert neurologist.
The inclusion criteria were as follows: 1) Having a migraine history since 4–5 years or more and recurrent migraine attacks for one year duration (at least 12 attacks per year); and 2) Having migraine attacks, when participating in the study. The frequency of migraine attacks was determined for each migraine patients. The high frequency of the migraine attacks was defined as more than 10 attacks per month [18].
Control group included 50 healthy subjects, age and sex-matched to the patient group. The sample size was determined with the confidence level of 90 percent. In addition, this study was approved by the Institution Ethics Committee, of the Isfahan University of Medical Sciences (Ir. May. Rec. 1395.3.405) and consent form was signed by all participants.
Dietary assessment
Dietary intake of the participants was assessed by an expert Nutritionist, using a valid semi-quantitative 168-item food frequency questionnaire (FFQ) [19]. Usual dietary intake was assessed using a validated 168-item semi-quantitative FFQ. A trained dietitian administered all the questionnaires. The questionnaire consisted of a list of foods with standard serving sizes commonly consumed by Iranians. Participants were asked to report their frequency of consumption of a given serving of each food item during the previous year on a daily (e.g., bread), weekly (e.g., rice, meat), or monthly (e.g., fish) basis. The reported frequency for each food item was then converted to a daily intake. Portion sizes of consumed foods were converted to gram using household measures. Total calorie and nutrients intakes were calculated using Nutritionist version 4 (N4) software (Tinuviel Software, Warrington, UK).
Statistical analysis
Data were analyzed by SPSS software (version 18;SPSS, Chicago, IL, USA). Independent sample t-test was used to compare thiamine intake between different groups, i.e., migraine patients and healthy subjects, or 2 migraine patients based on frequency of headache. Thiamine intake had been adjusted for energy intake, using analysis of covariance. The p value less than 0.05 was defined as statistically significant.
RESULTS
Fifty patients with migraine (12 men and 38 women) and fifty healthy people (12 men and 38 women), were enrolled in the study, as the case and control groups, respectively. Mean of the participants' age, weight, height, and body mass index was 35.1 ± 9.8 years, 65.3 ± 10.4 kg, 162.5 ± 8.4 cm, and 24.7 ± 4.0 kg/m2, respectively.
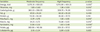
Dietary intake of the energy, thiamine, folate, and fat were significantly lower, among migraine patients than the healthy people (p < 0.001) (Table 1). However, the intake of energy-adjusted thiamine was not significant between case and control groups (p = 0.410) (Table 2).
Table 1
Demographic and dietary characteristics in migraine and healthy subjects
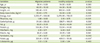
All values are expressed as mean ± standard deviation.
*p value < 0.05 considered as significant level.
![]()
Table 2
Difference of dietary intake* between case and control group or according to the different frequency of headache attacks

Value is expressed as means ± standard error.
*Adjusted for energy intake; †p value < 0.05 considered as significant level.
![]()
Patients with the high frequency of migraine attacks, showed significantly lower thiamine intake than the moderate frequency group (p = 0.010) (Table 3), while intake of the energy-adjusted thiamine was not significantly different, between high and moderate frequency groups (p = 0.240) (Table 2).
Table 3
Comparison of dietary intake in patients with the different frequency of headache attacks
All values are expressed as mean ± standard deviation.
*p value < 0.05 considered as significant level.
![]()
DISCUSSION
The current study showed that mean of thiamine intake among migraine patients is lower than the healthy subjects.
Migraine is a complex disabling neurological disease, and is accounted as 19th reason of disability during life, based on The World Health Organization report [20]. This disease imposes high health care cost to the patients, and has a substantial negative effect on the patient's quality of life [2122].
The B vitamins group contains several substances that may help prevent or threat migraine. Regular supplementation may have additional benefits in lowering the incidence of migraine attacks [23].
Vitamins also act as antioxidants and work effectively in oxidative stress to slow down the disease progression. B vitamins group is one of more concerns, however exact mechanism of thiamine deficiency in the pathogenesis of migraine is not clearly understood.
The etiology of migraine is multifactorial, with genetic components and environmental interactions considered to be the main causal factors. Some researchers postulate that deficits in mitochondrial energy reserves can cause migraine [24].
At the other hand, some studies have shown an association of hyperhomocysteinemia with migraine as well as the roles of vitamins B6, B9, and B12 in lowering the levels of homocysteine in patients with hyperhomocysteinemia [122526]. There is also evidence that riboflavin (vitamin B2) reduces the frequency of migraine attacks [24].
Thiamine helps the body produce cellular energy from food and is essential for the functioning of several enzymes in mitochondria, the cells power center. Despite the role of mitochondria in neural energy production, little direct research has been conducted on thiamine and migraine [23].
Mean of thiamine intake was significantly different between patients with the moderate and high frequency of migraine attacks. However, the differences was not significant, after adjusting for energy.
In addition, one of the hypotheses related to thiamine-migraine association is a mitochondrial dysfunction theory. Thiamine, as an important coenzyme in energy production (Krebs cycle), in mitochondrial metabolism, may related to migraine disease. Mitochondrial dysfunction, leading to oxygen metabolism impairment may associate with migraine pathogenesis [27]. Studies suggest that B vitamins group may involve in aerobic respiration reactions, which may relate to the migraine prophylaxis [2628].
In addition, thiamine has an important role in neuronal cells. Thiamine gets involved in neuro degeneration preventing and its deficiency results in apoptosis and severe cellular deficit [2930].
Few studies have investigated a relation between thiamine status and migraine headache. In the current study, we failed to find a significant difference between thiamine and energy intake, with the frequency of migraine attacks, while Prakash et al. [16] reported 2 female patients with chronic migraine, having a low blood thiamine concentration, in which thiamine supplementation led to a migraine attacks frequency reduction. The interrelation between migraine and thiamine deficiency is unknown, however Prakash et al. [16] suggested nausea, vomiting, and anorexia of migraine may lead to mild to moderate thiamine deficiency.
However similar studies, assessing other B vitamins group supplementation approved our results. Conflicting findings may be due to differences in daily dietary intake, physical activity, mental states, and genetic factors of the participants.
To support results of the previous studies, the low blood level of B vitamins group can be caused by the low food intake which occurs due to gastrointestinal disorders, such as vomiting and nausea, in migraine patients [16].
Hyperhomocysteinemia is caused by abnormal methionine biosynthesis due to deficiencies in folate, vitamin B12, and vitamin B6. Also, Menon et al. [31] showed that the supplementation of pyridoxine, folate and cobalamin could not be effective on the frequency of migraine attacks, while Lea et al. [12] reported that the intake of pyridoxine, folate and cobalamin led to low frequency of the migraine attacks.
To the best of our knowledge this is the first case control study about dietary intake of thiamine in migraine patients in Iranian people. In addition, adjusting for the dietary intake of energy led to increasing reliability of results.
There are several limitations that should be taken into account, when interpreting our findings. First, the sample size was not particularly large, which may lead to insufficient power, to detect the thiamine-migraine association. Secondly, although thiamine intake was assessed by 168-item FFQ that was validated with the same population, recall bias cannot be excluded. Third, subjects were collected from a single hospital and the generalization of the findings is limited.
CONCLUSION
Our findings cannot suggest a significantly lower thiamine intake, among migraine patients, compared to the healthy people. The same conclusion was achieved, regarding patients with the high frequency of migraine attacks, compared to moderate group. Considering the safety, well-tolerated properties and cost-effectiveness of thiamine supplement, it is reasonable that more investigations should be conducted, before excluding thiamine supplementation as a potential efficient treatment for migraine. Randomized controlled trials are needed to prove this result.
 XML Download
XML Download