

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Skin cancer is the most common type of cancer in the United States [1]. Non-melanoma skin cancers including squamous cell carcinoma (SCC) and basal cell carcinoma (BCC), represent the most frequently malignant neoplasms in Caucasians [2]. There is similar prevalence in Iran which skin cancer with about 15% of all cancers, is the most common and BCC is the frequent morphologic type of skin cancer [3]. Although the mortality rate of BCC is extremely low, it represents a significant health care burden with major morbidity and cosmetics problems [4].
Constitutional risk factors for BCC development have been proposed as skin color, age, sex, skin phototype (I, II), frequent sun exposure and sunburn, severe actinic damage, history of radiotherapy, and etc.[5]. Apart from ultraviolet radiation (UVR) exposure, dietary factors including dietary lipids are also involved in the development of skin cancer [6].
Several studies have reported different changes in the fatty acid composition of red blood cell (RBC) in patients with various types of cancer [7]. The structure and function of erythrocytes have been proposed as cellular biomarker in inflammatory disorders. It has been indicated that the fatty acid composition of RBC membranes may reflect fatty acid composition in other body tissues and the fatty acid composition of RBCs especially reflects the composition of fatty acid intake during the cell's life time of about 120 days [8910]. Different effects of individual fatty acids on expression of genes concerned in multiple biologic pathways, including inflammation and oxidative stress have been reported [11]. Furthermore, prospective studies have been investigated the circulating fatty acids levels and the risk of different type of cancers [1213].
Polyunsaturated fatty acids (PUFAs) taken up into human skin [14], may affect UVR-induced immunosuppression through different mechanisms, including effect on membrane fluidity, signal transduction, transcription-factor activation and soluble mediator production [15]. High levels of n-6 fatty acids are also associated with specific deleterious immune responses such as elevation of prostaglandin E2 (PGE2) levels, with aggressive growth of keratinocytic skin cancer in humans [16]. On the contrary of n-6 PUFAs effects, n-3 PUFAs could increase latency of tumor and decrease tumor numbers in early promotional cancer stages [16]. Blood n-3/n-6 ratio plays a fundamental role in the general consequence of skin photocarcinogenesis [16]. Increasing risk of breast, prostate, or colorectal cancer has been reported to be associated with increasing concentrations of some individual trans-monounsaturated fatty acids (MUFAs) [12].
In the current study, we explore the fatty acid composition of RBCs including PUFAs and MUFAs concentration and suggested ratios to find out probable differences between BCC patients and control group.
MATERIALS AND METHODS
Study design and participants
The survey was approved by ethical committee of Tehran University of Medical Sciences (TUMS) and all patients were fully informed of the purpose of the study and gave their informed consent to participate in the study (ethical approval number: IR.TUMS.REC.1394.635). This hospital-based case-control study was performed on newly diagnosed BCC patients between April 2010 to February 2013 in 3 year-duration, who their disease histopathologically confirmed by dermatologist in contact time in Razi Hospital, Tehran, Iran. The control subjects were selected from first-visit outpatients without any history of skin cancer. Patients who are on supplements and vitamins, previous systemic disorder other than skin cancer like diabetes mellitus were excluded. For controlling confounding factors also both groups were matched on age and body mass index (BMI). All the procedures were done based on Declaration of Helsinki. Trained interviewers systematically collected and checked information from the questionnaires and contacted the participants to describe the study and invite them.
Sample size calculation
Sample size was measured according to type 1 (α) and type 2 errors (β) as 0.05 and 0.20 (power = 80%), respectively and based on the previous study [13]. Standard deviation (SD) and difference in mean or effect size (d) of fatty acids in RBC membranes were considered as 1.04 and 0.78, respectively as the key variables. Although we needed 28 subjects in each group but because of possible dropouts 80 participants were interviewed for the study, 40 cases and 40 controls.
Data collection
Face to face interview for demographic characteristics, and drug and medical history was performed for all 80 subjects. Stadiometer Seca 700 (Seca GmbH, Hamburg, Germany), which was attached to the wall, was used for height measurement. All subjects were asked to stand looking straight with shoulders, back of head, heels, and hips next to the wall. Weight of participants was measured by Seca digital scale model 700.
Dietary assessment
All subjects completed two 24-hour dietary recalls by nutritionist's help which included 2 randomly selected days (week day). The dietary recalls were analyzed using Nutritionist IV software (First Databank, San Bruno, CA, USA) adjusted for Iranian foods.
Reagents and standards
BF3-methanol 14%, sodium sulfate and sodium chloride standards were obtained from Sigma-Aldrich (St. Louis, MO, USA). Analytical grade chloroform, methanol and n-hexane were acquired from Merck (Darmstadt, Germany). Thirty-seven fatty acid methyl esters (FAME) Mix standards, were provided from Supelco(Bellefonte,PA, USA). Water was purified and filtered to reach a resistivity 18.2 MΩ·cm at 25°C and TOC value < 5 ppm through a Milli-Q Plus system filter (Millipore, Bedford, MA, USA).
Fatty acids extraction, purification, and preparation of FAME
Ten mL of fasting venous blood were obtained in an ethylenediaminetetraacetic acid (EDTA) bottle and centrifuged at 1,500 revolutions per minute for 5 minutes to separate the erythrocytes. The erythrocytes were rinsed 3 times with phosphate buffered saline (PBS) to eliminate iron of hemoglobin to avoid oxidative degradation of fatty acids. All RBCs were reserved in 500 μL microtubes in −80°C for gas chromatography measurement. After each sample of RBCs was thawed to room temperature, the lipids were extracted from the erythrocytes with 2:1 (v/v) chloroform-methanol by Folch et al. [17] method and then centrifuged at 1,500 × g for 10 minutes. FAME preparation was performed by BF3-methanol 14%. So, 200 μL of dried RBC samples (evaporation by nitrogen gas for better methylation of fatty acids), 2 μL BF3-methanol 14% and 1 μL methanol were incubated for 10 minutes at 60°C [18]. Two mL of N-hexane solution was added to the samples and were stirred by Vortex (Middleton, WI, USA) for 10 minutes. The upper layer was reserved, drown off into a vial.
Gas chromatography and fatty acids quantification
Gas chromatography analyses were done by a 6500GC Young Lin (Anyang, Korea) instrument with auto-sampler, a split/splitless injector, flame ionization detector (FID), and a hydrogen gas generator. Separation of FAME was completed on a TR-CN100 column (Teknokroma, Anlítica, SA, USA) (37 FAME MIX-MS detector: 60 m × 0.25 mm × 0.20 μL; Standard: 1 μL FAME MIX in methylene chloride; Injection: 280°C, split 20:1). Hydrogen was used as carrier gas, constant flow mode; 1 μL in splitless mode and 24 PSI was injected. The temperature of the injector and the FID were 280°C. Inlet temperature 240°C, split 40:1, and injection 0.20 μL. The initial temperature of the oven was 90°C for 5 minutes then to 220°C at 4°C/min to 1°C/min for another 5 minutes, and finally the temperature increased to 240°C: 4°C/min for total of 47.5 minutes. Quantification of the extracted methyl esters of fatty acids was completed by use of a mixture of the Supelco standards. Calibration was performed by standard (Supelco) which has 37 fatty acids in 2%, 4%, and 6%. Four solutions of increasing concentration (0.3, 0.2, 0.1, and 0.05 ppm) of the mix of standards (Teknokroma) were prepared; each solution was analyzed 3 times and the resulting chromatograms were used to make the calibration curve for all component of the mixture. The computer program was planned to measure the area under every peak and various peaks representing different fatty acids. The percentage of each fatty acid was revealed from the percentage of each peak area in comparison to the total peak area.
Data analysis
Distribution of demographic characteristics, food intakes and serum lipid were compared between BCC patients and healthy people. Independent t-test was used for continuous variables and distribution of variables was evaluated by Kolmogorov-Smirnov test. Means of dietary intakes were adjusted for age, BMI, and gender. All values were demonstrated as mean ± standard error of means (SEMs). If p value was less than 0.050 in any analysis, it was considered statistically significant.
RESULTS
The mean ages of the BCC patients and control group were 57.76 ± 1.56 and 54.05 ± 1.16 years, respectively. As presented in Table 1, the demographic characteristics of participants were not significantly different between 2 groups (p > 0.050).
Table 1
Demographic characteristics and medical history of healthy and BCC group

Values are presented as number of patients (%) or mean ± SEMs.
BCC, basal cell carcinoma; BMI, body mass index; SEM, standard error of mean.
*p value is reported based on independent Samples t-test; †p value is reported based on χ2 test.
![]()
Dietary intake analysis shows that energy, macronutrients (total fat, protein, and carbohydrate) and micronutrients (selenium, copper, zinc, beta carotene, α-tocopherole, and molybdenum) intakes were not significantly different between patients and control groups. Furthermore, intakes of various types of fats were not significantly different between BCC and control groups (Table 2).
Table 2
Energy, macronutrients, and micronutrients intakes of BCC subjects and control group
Values are presented as mean ± SEMs.
BCC, basal cell carcinoma; SFA, saturated fatty acid; MUFA, monounsaturated fatty acid; PUFA, polyunsaturated fatty acid; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; SEM, standard error of mean.
*p value is reported based on independent Samples t-test.
![]()
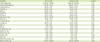
MUFA concentration of RBC membranes
Table 3 represents MUFAs concentration of RBC membranes. Among all MUFAs, heptadecenoic acid (p = 0.010) and oleic acid (p < 0.001) were significantly higher in BCC patients in comparison with control group. There were no significant differences among other MUFAs in BCC patients compared with control group (p > 0.050).
Table 3
MUFAs and PUFAs of RBC membrane in BCC subjects and control group

Values are presented as mean ± SEMs.
MUFA, monounsaturated fatty acid; PUFA, polyunsaturated fatty acid; RBC, red blood cell; BCC, basal cell carcinoma; LA, linoleic acid; AA, arachidonic acid; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid; SEM, standard error of mean.
*pvalue is reported based on independent Samples t-testand less than 0.05 was considered statistically significant.
![]()
PUFA concentration of RBC membranes
PUFA concentrations of RBC membranes were shown in Table 3. Compared to the control group, BCC patients had a higher linoleic acid (LA) and arachidonic acid (AA) (p < 0.001). There were no significant differences among other PUFAs in RBC membranes of BCC patients in comparison with control group (p > 0.050).
Practical ratios between fatty acids of erythrocytes membranes
Table 4 represents fatty acid product to precursor ratio and practical ratios between fatty acids of erythrocytes membrane in case and control groups. It has been indicated that n-3 was significantly lower (p = 0.040) and n-6 was significantly higher (p = 0.002) in BCC patients. We also explored other ratios which have been investigated in previous studies [19]. N-3 highly unsaturated fatty acids (HUFAs) (p = 0.670), n-6 PUFAs/n-3HUFAs (p = 0.450), AA/eicosapentaenoic acid (EPA)20:4n-6/20:5n-3 (p = 0.130), AA/docosahexaenoic acid (DHA) 20:4n-6/22:6n-3 (p = 0.810) and n-3/n-6 fatty acids (p = 0.310) were not significantly different between groups but total PUFAs (p < 0.001) and n-6 PUFAs/n-3 PUFAs (p = 0.002) showed significant differences between BCC patients in comparison with control group (Table 4).
Table 4
Fatty acid product to precursor ratio and practical ratios between fatty acids of RBC membrane in BCC subjects and control group

Values are presented as mean ± SEMs.
RBC, red blood cell; BCC, basal cell carcinoma; PUFA, polyunsaturated fatty acid; HUFA, highly unsaturated fatty acid; AA, arachidonic acid; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid; SEM, standard error of mean.
*p value is reported based on independent Samples t-test and less than 0.05 was considered statistically significant.
![]()
DISCUSSION
In the present case-control study, alterations of fatty acid profile in the erythrocytes membranes were indicated in BCC patients compared with healthy control subjects. Levels of heptadecanoic acid, LA, oleic acid, and AA, were significantly higher among BCC cases compared with controls. Other MUFAs and PUFAs were not significantly different between 2 groups. On the other hand, n-6 fatty acids were significantly higher (p < 0.001) and n-3 fatty acids were significantly lower (p = 0.040) in BCC patients compared with controls. However, n-3 to n-6 ratio were not significantly different between groups (p = 0.310).
Some of the earliest evidence of the skin cancer in animal model has reported that dietary fat acts as a tumor promoter with specific types of fat exert defined carcinogenic effects [20]. There are considerable differences in the amount of fat intake (energy intake, %) and the ratios of saturated fatty acid (SFA): MUFAs and PUFAs between Japanese, Mediterranean, and American diets so this diversity could be related to their disease prevalence, including cancers in several sites [19]. Because animal evidence showed that lower total energy intakes reduce carcinogenesis [20] we wanted to ensure that energy intake did not differ between groups. However, as shown in Table 2, dietary intake analysis indicates that energy, macronutrients and micronutrients (selenium, copper, zinc, beta carotene, α-tocopherole, and molybdenum) intakes were not different in patients and control groups. Furthermore, there were no significant differences between BCC and control group regarding various types of fatty acid intakes (Table 2).
Carcinogenic effect of higher levels of AA have been reported because of its role in eicosanoids metabolism [21]. It has been suggested that AA metabolism implicated in metastasis pathogenesis thorough cell-matrix interactions and integrin signaling [22]. Harris et al. [20] reported higher risk of SCC with higher levels of AA and PUFA/SFA ratio of RBC membranes. They reported that possible inflammatory response of AA to UVR could be associated with higher SCC risk.
The higher composition of 18:2 n-6 and n-6 PUFAs were associated with increased risk for prostate cancer and breast cancer, but that of AA had no association [19]. Animal studies indicate that n-6 PUFA increase carcinogenesis [23]. Adds to evidence from animal studies, our results are consistent with a case-control study which reported a significantly higher risk of SCC with greater AA concentrations in erythrocytes membranes [20]. Our results in BCC patients are consistent with other studies representing low levels of n-3 PUFAs in erythrocytes membrane in patients with gastrointestinal cancers [24].
The n-3 and n-6 PUFAs share the same enzymes and there is competition between the 2, being as substrates for cyclooxygenase (COX) and lipoxygenase (LOX) enzymes. So, the formation of different prostaglandins (PGs) and leukotrienes could be occurred based on substrates like PGE3 from n-3 PUFA which found to exert anticancer effect instead of PGE2 from n-6 PUFA which promote cancer development. These results also proved in the human and mouse skin after a single acute exposure to UVR. High levels of n-6 PUFA increase the levels of PGE2, an immunoregulator known to exacerbate UVR-carcinogenesis with aggressive growth of keratinocytic skin cancer [16]. The expression of COX-2 has been shown to be elevated in human SCCs and BCCs. N-3 PUFAs have been shown reduced ultraviolet B (UVB; UVB-medium wave), together with ultraviolet A (UVA; long wave) and ultraviolet C (UVC; short wave) but UVB is more potent and the main culprit in carcinogenesis and skin cancer) erythemal sensitivity, maybe by decreasing UVR-induced PGE2 level in the skin and reduction of interleukin (IL)-1α, tumor necrosis factor (TNF)-α, and IL-6 levels [25].
A decrease in risk of SCC with increased intake of diets with a high n-3/n-6 ratio was reported in a population-based case-control study [20]. Ratio of n-3/n-6 in circulation plays a key role in determining the overall effect on skin photocarcinogenesis [23].
Despite consistent in vitro and animal studies for the role of n-3 and n-6 fatty acids in cancer, human evidence of these effects is controversial. This lack of consistency was highlighted in our analyses, where there was no significant difference in n-3/n-6 ratio in BCC patients in comparison with control group. A large prospective study also failed to show a reduction in BCC risk with high n-3 fatty acid intake over the 8 years of follow-up [26] and based on our best knowledge this is the first report of fatty acid contents in RBCs of BCC patients. However, unexpected associations with heptadecenoic acid, MUFAs, were identified which was not reported before that time to be changed in skin malignancy.
In our study oleic acid was also significantly higher in RBC membranes of BCC patients in comparison with healthy control. Other studies in colorectal adenoma also reported increased levels of oleic acid in erythrocytes membranes [26]. Similarly, a case-control study in Japan reported the same association [27]. Because of endogenous synthesis of oleic acid, elevated level of oleic acid, as previously reported in relation to colon [27], gastric [28], and to breast cancer risks [29] could be resulted from increased endogenous synthesis from stearic acid rather than to a diet rich in oleic acid. Also, it must be noted that abundant amounts of oleic acid are found in numerous cancer cells serves as signal transduction mediators and cellular differentiation [27]. Because of increased expression of stearoyl-CoA desaturase-1 (Δ-9-desaturase) in several human cancers [30], our data may suggest that endogenously synthesized oleic acid, act as regulators of cancer cell growth in BCCs.
Some limitations and strengths of the study should be acknowledged. The first strength of study is that individual fatty acids were measured on pretreatment blood samples. Also, to increase the statistical power, we randomly selected the control subjects, who were matched for age and BMI. Next, we excluded control subjects with any diseases associated with lipid metabolism. It was reasonable to assume that our control subjects come up within population base. Our initial protocol stipulated an alpha level of 0.05 to decrease the available statistical power and in order not to increase the likelihood of a type II error. However, there are some limitations that must be mentioned. We cannot rule out possibility of all confounding bias. Lack of information on non-steroidal anti-inflammatory drugs, and their effect on COX-2, thus, when investigating the associations between n-6 and n-3 PUFAs, we cannot adjust for this potential confounding factors in our study. At last, the sample size, the number of cases and controls was not large enough to thoroughly assess the associations in subgroup analyses.
In conclusion, there is a need to comprehend the etiology of the various skin cancers to identify modifying risks, and to expand efficient intervention strategies. Other strategies rather than minimizing UV exposure are needed. In accordance with rodent models of photocarcinogenesis, our study provides evidence that lipids are important in BCC development in human skin. This study supports the hypothesis that AA metabolism is involved in the promotion and/or progression of skin cancers in humans. But it is not clear if these findings are due to AA solely or with other fatty acids. Therefore, we hope future studies to consider dietary factors that can significantly affect skin cancer.
 XML Download
XML Download