

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gestational diabetes mellitus (GDM, approximately 5% of pregnancies) is considered as an important risk factor for development of later-onset DM [1]. Diabetes affect nearly 1% to 14% of pregnancies of which 3% to 5% are GDM [234]. GDM has been reported to be associated with high risk of developing type 2 diabetes later in lifetime, metabolic syndrome, and cardiovascular disease. For example, the prevalence of metabolic syndrome in GDM women is 3 times higher than in women with normal glucose tolerance during pregnancy [5].
In diabetic condition, several factors such as glucose oxidation, alterations in antioxidant defense system, lipid peroxidation, non-enzymatic glycation of proteins and following oxidative destruction of glycated proteins could result in production of free radicals [678]. Imbalance between the formation and inactivation of oxygen free radicals cause oxidative damage, which is associated with the destruction of membrane lipids and production of lipid peroxides and their products. Antioxidants which have low molecular weight, remove reactive oxygen species (ROS) [9]. Usually, enzymatic and non-enzymatic antioxidants act via natural antioxidant mechanism in the human body, similarly fruits and vegetables containing antioxidants may neutralize all kinds of free radicals [10]. Total antioxidant capacity (TAC) demonstrates the balance between antioxidants (neutralizing systems) and the oxidants (oxidative stress). Antioxidants such as catalase, superoxide dismutase, β-carotene, vitamin C, vitamin E, and glutathione peroxidase (GPX) are known to protect from the adverse action of ROS and their derivatives [11]. Some investigators have reported increased lipid peroxidation and significant depletion in antioxidant capacity during the development of gestational diabetes [12].
On the other hand, it was reported that nutrients could influence oxidative stress by rising or reducing ROS or acting substrate for free radicals and by antioxidant roles [1314]. Several studies have reported that levels of antioxidants such as selenium, zinc, and vitamin E were reduced in GDM [121516]. Furthermore, several studies have found that a diet rich in antioxidants promotes better health and enhances the total antioxidant status (TAS) [13]. However, studies about the maternal nutrition status and antioxidant nutrients and TAC in women with GDM are limited. This study aimed to compare maternal nutrition status and TAC in women with GDM and in healthy pregnant women.
MATERIALS AND METHODS
This case-control study was performed in 80 pregnant women, comprising 40 women with definite diagnosis of GDM, and 40 healthy pregnant women (healthy group) that attended at the Department of Obstetrics and Gynecology of the Shahid Beheshti Hospital in Isfahan, Iran, from February until August 2016. GDM was defined if 2 or more of the 100 g oral glucose tolerance test (OGTT) glucose levels exceeded the American Diabetes Association (ADA) criteria [17]: fasting, ≥ 95 mg/dL (5.3 mmol/L); 1 hour, ≥ 180 mg/dL (10.0 mmol/L); 2 hours, ≥ 155 mg/dL (8.6 mmol/L); 3 hours, ≥ 140 mg/dL (7.8 mmol/L). It was approved by the Research and Ethics Committee of Isfahan University of Medical Sciences (IRB No. 1394.3.889). Overall, 80 pregnant women at 24–28 weeks of gestation were allocated. Gestational age was confirmed in all pregnant women by a routine ultrasonographic examination performed during the first trimester of gestation.
After obtaining written consent, eligible women who met study inclusion criteria according to their blood sugar level entered the study. Objectives and methods of study were explained to participants, and data forms including demographic and obstetrics details were completed by interview. Dietary intakes were collected by a validated 168 items semi-quantitative food frequency questionnaire (FFQ) developed in Iran [18]. This questionnaire was administered to determine frequency of food consumption during pregnancy and ask about the average frequency of intake of during last year. Information of FFQ was extracted by Nutritionist-4 software (First Data Bank Inc., Hearst Communications Inc., San Bruno, CA, USA) by a dietitian. A team of skilled gynecologist and dietitians conducted the study under standard protocols.
For control group, subjects were excluded if they were taking medication and smokers, those with other medical conditions such as high blood pressure and family history of DM. The pregnant women were also asked about history of prenatal multivitamin/mineral supplements intake.
Body height and pre-pregnancy weight of the subjects were asked to calculate their body mass index (BMI). Also, weight gain during pregnancy was recorded. Gestational weight gain was calculated as the weight measured at glucose screening test minus prepregnancy weight. The 2 groups were matched based on gestational and maternal age and BMI.
TAC was determined from the sera that was frozen at −70°C and measured by using a double antibody sandwich enzyme-linked immune-sorbent assay (ELISA).
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) (version 18.0; SPSS Inc., Chicago, IL, USA) software. Continuous variables are presented as the mean and standard deviation (SD). Multivariate logistic regression was performed to compare independent variables and other potential risk factors in the 2 groups. A p value less than 0.05 was considered significant.
RESULTS
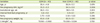
The demographic and anthropometric characteristics of GDM and non-GDM are presented in Table 1. There were no significant differences about age, number of pregnancies, gestational age, interval from last pregnancy, pre-pregnancy BMI, pre-pregnancy weight, and weight gain between the groups. Also, there were no significant differences in education level (45% writing, 55% diploma in diabetic group vs. 40% writing, 60% diploma in control group). All women were taking multivitamin and minerals supplements routinely used during pregnancy.
Table 1
Comparisons of demographic and anthropometric characteristics of women with GDM or Non GDM
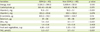
Based on the results obtained from the dietary intake questionnaire, the mean energy intake was not significantly different between GDM and healthy mothers (2,536.3 ± 390.2 vs. 2,669.4 ± 321.8 kcal). Dietary intake of vitamin E (11.8 ± 3.1 vs. 16.2 ± 3.1 mg), selenium (81 ± 26 vs. 95 ± 36 µg), zinc (7.4 ± 1.9 vs. 9.1 ± 1.7 mg) in GDM were significantly lower than non-GDM group. The groups had no statistically significant differences in vitamin C (223.2 ± 131.8 vs. 235.1 ± 122 mg), β-carotene (803.2 ± 512.1 vs. 1,009.1 ± 634.7 µg), copper (1.4 ± 0.6 vs. 1.5 ± 0.6 mg), and fruit and vegetable intake (4.90 ± 1.01 vs. 5.30 ± 1.10 cup) (Table 2). Serum levels of TAC in GDM were significantly lower than healthy pregnant women (2.3 ± 0.7 vs. 3.7 ± 0.1 µmol/L; p < 0.001).
Table 2
Comparison of dietary nutrient of women with GDM or Non GDM
Multivariate logistic regression analysis showed that TAC, vitamin E, and zinc intakes were significantly associated with the risk of GDM. For every unit increase in TAC, the odds of GDM were reduced by 9.6 fold. It was also found that for every unit increase vitamin E intake, the odds of GDM were reduced by 1.5 fold. In addition, for every unit increase in zinc intake, the odds of GDM were reduced by 1.7 fold (Table 3).
Table 3
Multiple logistic regression analysis of GDM predictors

DISCUSSION
In the present study, we observed that intakes of several micronutrients including vitamin E, selenium and zinc were significantly lower in women with GDM as compared to healthy pregnant women. Previously, Ceriello et al. [19] assessed the effect of vitamin E intake which is known to have antioxidant properties on glycohemoglobin (GHb) concentrations in diabetic individuals. In that study, they suggested beneficial effects of large doses of tocopherol orally administered to diabetic individuals with low GHb concentrations. Low levels of plasma vitamin E along with significant decrease in GPX has been reported to be in favor of the overwhelming of antioxidant defense systems [20]. However, the observed associations were conflicting. Several studies have reported decrease of vitamin E in GDM [202122], however, other studies demonstrated rise in vitamin E level during GDM [2324].
In this study, we found no significant differences in intakes of vitamin C, β-carotene, and copper between GDM group and healthy group, whereas significant difference was observed in selenium intake between the groups. This suggested appropriate intakes of dietary vitamin C, β-carotene and copper based on recommended allowance in the management of GDM [25]. Also, the results are in agreement with previous studies, reporting no significant differences in intake of vitamin C and β-carotene in GDM patient [26]. With regard to selenium, Molnar et al. [27] documented significantly reduced levels of serum selenium in GDM. However, conflicting findings have shown that women who consumed < 70 mg of vitamin C daily were at a 1.8-fold increasing risk of GDM as compared with women who consumed higher amounts [28] and in another study, concentrations of vitamin C significantly increases in women with GDM [29].
Also, we observed that dietary intake of zinc is significantly lower in gestational hyperglycemia women. This is in line with the previous result [16] that intakes of zinc were negatively associated with gestational hyperglycemia and daily intake of zinc, 1 mg per day, caused 11% reduction in the risk of gestational hyperglycemia. It is conceivable that zinc could limit oxidant-induced damage with protection against vitamin E depletion, thereby increase the stabilization of membrane structure, restriction of endogenous free radical production, contribution to the structure of the antioxidant enzyme extracellular superoxide dismutase, maintenance of tissue concentrations of metallothionein, as a possible scavenger of free radicals. It was reported that mild zinc deficiency in rats can exhibit high serum levels of ceruloplasmin, the acute phase protein. High concentration of this protein may be a sign of inflammation, which is associated with above-normal phagocyte secretion rates of free radicals [30]. However, another study reported no association between low maternal intake of zinc and GDM [31].
It was previously reported that consuming the highest intake (1.35 servings) a day of green leafy vegetables as compared with lowest intake (0.2 servings) resulted in a 14% reduction in risk of type 2 diabetes [32]. Bagheri et al. [33] also suggested that fruits and vegetables consumption was significantly lower in GDM compared to control group, therefore, fruits and vegetables can help reducing the risk of diabetes in pregnant women. In contrast to the previous findings, there were no significant differences in fruit and vegetables consumption between GDM and healthy pregnant women, which requires further confirmation in other studies.
Antioxidants are known to play protective roles against oxidative stress. TAC indicates the balance between the neutralizing systems and oxidative stress [11]. In our study, we observed low levels of serum TAC in women with GDM as compared to healthy group, similar with other studies [1634]. Karacay et al. [35] demonstrated that TAS levels in women with GDM were notably lower than those in non GDM. Also, Suhail et al. [12] showed a significantly lower level of antioxidant capacity throughout the development of GDM. In another study, mothers with GDM had higher content of lipoperoxidation products and malondialdehyde (MDA), biomarkers of oxidative stress [20]. Several mechanisms can be speculated for generation of free radical at higher glucose concentration in pregnancy. It includes non-enzymatic protein glycation that may induce production of oxygen free radicals [36], increased mitochondrial electron transport chain flow, oxidative activities of the fetus [37]. The increased oxidative stress in GDM is caused by increased levels of free radicals and deficiencies in antioxidant defense systems [13839]. This may explain why we found low TAC in our pregnant women with GDM.
There are some limitations in the current study that should be considered cautiously. The sample size of study was small and our study did not provide information about serum micronutrient concentrations. However, this study has strengthened by the close matching of control subjects against GDM subjects. Subjects were matched based on gestational, maternal ages, and BMI, thus negating these parameters as confounders. Also, subjects were carefully interviewed by a dietitian about demographic data and dietary intakes were compared by questionnaires filled by a dietitian.
In conclusion, our results suggest that antioxidant status could be enhanced by consumption of food rich in antioxidant and high dietary intake of fruit and vegetables and other rich antioxidant sources in GDM, which may be ultimately beneficial in the prevention and management of GDM.
 XML Download
XML Download