

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The benefits of physical activity for health maintenance have been well documented, especially in the prevention and management of chronic diseases such as some cancers, type 2 diabetes, and cardiovascular disease [12345]. In this context, accurate measurement of physical activity and energy expenditure is essential both in epidemiological studies and in assessment of intervention programs' efficacy [6]. In clinical setting, assessment of energy expenditure allows to estimate nutrient requirements for patients during nutrition support [7].
Physical activity is defined as any bodily movement produced by skeletal muscles that results in energy expenditure [8]. It is important to emphasize that the physical activity and energy expenditure are 2 different concepts. Simply stated, physical activity is a behavior that results in an elevation of energy expenditure above resting levels [9]. Total energy expenditure (TEE) refers to the total amount of energy expended during a 24-hour period, and it contains 3 main components: resting energy expenditure (REE), thermic effect of food (TEF), and activity energy expenditure (AEE) [10].
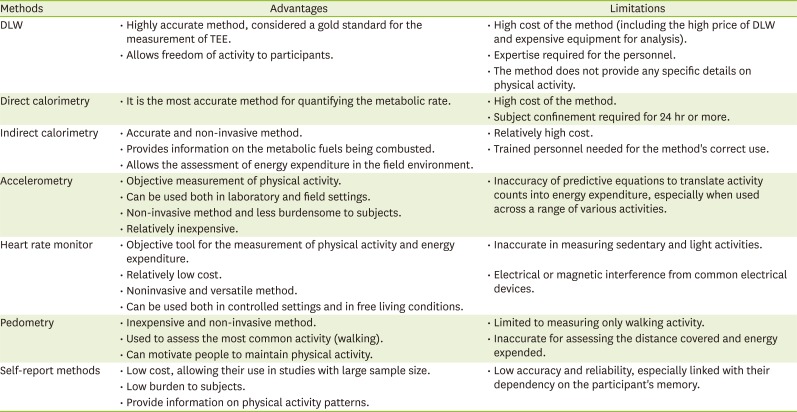
Various methods exist for assessing physical activity and energy expenditure, and each of them has advantages and limitations as summarized in Table 1 [6]. Understanding of these methods is important to decide which method to use for the specific study context. The purpose of this review was to discuss the components of TEE and present different methods of physical activity and energy expenditure assessment, with emphasis on each method's advantages and limitations.
Table 1
Advantages and limitations of different methods for physical activity and energy expenditure measurement
COMPONENTS OF TEE
REE
The REE, the largest portion of TEE, is the energy required to maintain the basic metabolic activities including maintaining the body temperature and keeping the functioning of vital organs such as the brain, the kidneys, the heart, and the lungs. REE is defined as the energy expended by a fasting person at rest, in a thermo-neutral environment. Factors most significantly affecting the REE include body composition, gender, body temperature, age, energy restriction, and genetics and endocrine system [10]. A brief description of selected factors is presented here: (1) Body composition: fat-free mass (also called lean body mass) is the primary determinant of REE, meaning that high fat-free mass individual having higher REE [11]; (2) Gender: REE tends to be higher in males than in females [1213], and this may be due to the higher percentage of lean body mass in males compared to females [1014]; (3) Age: older individuals have lower REE compared to younger people [15]. The age-related decline in REE has been shown to be independent from changes in body composition, suggesting that additional metabolic changes may also be involved [1516]; and (4) Energy restriction: efforts to lose weight by restricting energy intake lead to a decrease in REE [17]. This phenomenon may explain the difficulty to maintain weight loss by low calorie diets, which is associated with the biological response to energy restriction [18].
The REE is measured when the fasting person is resting in a comfortable environment. The fasting time is usually about 2 to 4 hours [19]. REE is slightly higher (about 10%) than the basal energy expenditure (BEE), which is the lowest energy expenditure of person and measurement of BEE requires more stringent conditions. A person's BEE is determined when individual is in a post absorptive state (i.e., no food intake for at least 12 hours), is lying down (supine), and is completely relaxed (motionless)—preferably very shortly after awakening from sleep in the morning [19].
AEE
The AEE is the most variable among the components of TEE, both at the intrapersonal and interpersonal level. In sedentary people, it can account for less than half of BEE while it can be as high as 1 to 2 times the BEE or more in case of very active people such as some athletes or heavy laborers [20]. Factors that influence AEE include intensity, duration, and frequency of activity [6].
TEF
The TEF, also referred to as diet-induced thermogenesis (DIT), is the energy required for the food digestion, absorption, transport and metabolism, storage of nutrients, and elimination of wastes. It represents increase in energy expenditure above the REE, which can be measured for several hours after a meal. The TEF is estimated as about 10% of the daily TEE [10].
DOUBLY LABELED WATER (DLW) METHOD
Principle of the method
The DLW method uses stable isotopes of oxygen (18O) and hydrogen (2H) for the measurement of TEE. The DLW method is widely recognized as the gold standard for the measurement of TEE [21], and has been used in various studies to validate other methods [2223]. In addition to its high accuracy [24], the DLW method presents the advantage of its noninvasive nature and possibility for the subjects to continue their normal activities during the measurement period. The method also has a limited burden on subjects [25]. However, limitation of the method is its high cost due to the high price of DLW, the expensive equipment and expertise required for analysis [21]. Another limitation of the DLW technique is that it provides the overall measure of averaged daily TEE over the measurement period, but it does not provide any specific details on physical activity. Currently, this method has been used in a wide range of population categories including infants [2627], pregnant and lactating women [2829], and the elderly [2330].
The method is based on the following principle: after the subject ingests a dose of 2H218O, there is an equilibration of the 2 isotopes with total body water (TBW) followed by their elimination from the body, which occurs at different rates. Deuterium (2H) is lost from the body via only water (H2O) while 18O is lost both via water and carbon dioxide (CO2). The rate of CO2 production (rCO2) is calculated as the difference between the elimination rates of 2H and 18O, using the following formula [31]:
where ko and kh (day-1) are the elimination rates of 2H and 18O, respectively.
The TEE is calculated by using the modified version of Weir's formula based on rCO2 and food quotient (FQ) [31]:
Protocol of the DLW method
There are 2 basic protocols for the DLW method: the 2 point and the multi-point approaches. The 2-point protocol as the minimal form requires 3 specimens including a pre-dose baseline, a post-dose specimen taken on the day of dosing after the isotopes have equilibrated throughout the body, and a final specimen taken at the end of the study (that is, at day 10–14). The multi-point protocol as the most extreme form generally involves the steps taking a pre-dose baseline specimen and specimens every day after intake of the dose until the end of the sampling period. In practice, the 2 approaches have been modifications in the 2 approaches and they are quite similar [25].
Concerning the 2-point protocol, the most commonly used form is the modified approach in which a total of 5 samples are collected [133233]. Subjects are requested to come to the clinical site or urine sample collection center in the morning after an overnight fast, and the protocol begins by collecting the baseline urine sample. A short time after, the participant drinks the DLW prepared based on the subject's TBW [133233]. In some studies, the amount of isotope dose in DLW was determined by the participant's body weight [313435]. One hour after drinking the DLW, subjects should void to empty the bladder and the time must be recorded. However, this urine is not collected since the isotope equilibrium with the body water is not yet established at this time. Three and 4 hours after drinking the DLW, 2 more urine samples should be collected. The subject should not drink and eat between the 3 to 4 hours during urine sample collections to minimize any short-term effect of water intake on urine enrichment. On the final day of experimental period, 2 more urine samples should be collected at about the same time of the day before. Typical intervals between the initial and the final urine collections are 7, 10, or 14 days [25]. In the multi-point approach, more urine samples are collected after DLW administration than those in the 2-point protocol [343536]. During the study period, all samples must be collect at similar time to the previous days.
The number of urine samples collected is not a critical consideration with regard to the validity of the DLW technique. Rather, the choice of sampling frequency depends on the investigator's preference for precision of the method [25]. The 2-point protocol presents an advantage of using fewer samples, and provides the more exact estimate of TEE under conditions in which there is day to day variation in energy expenditure or water turnover. On the other hand, the multi-point protocol has the advantage of data averaging and thus minimizes the analytical error. In addition, it allows the investigator to assess the differences in energy expenditure for sub-periods within the metabolic period [25]. After urine samples collection and storage, analysis is performed by the isotope-ratio mass spectrometry method [25].
The dose of DLW
The dose of DLW is based on the body size of subject in order to match the body water enrichments to the isotope-ratio mass spectrometry precision. Considering the difficulty of measuring TBW, it must be estimated. In most DLW studies, investigators have assumed TBW as 60% of body weight. The 99 atom % deuterium (2H) and 10 atom % 18O are the most commonly used for enrichments of the labeled water available on the market. The International Atomic Energy Agency (IAEA) recommends doses of 0.12 g·kg−1 body water of 99 atom % deuterium labeled water and 1.80 g·kg−1 body water of 10 atom % 18O. When the more highly enriched 18O water is used, the dose should be reduced [25]. Prior to the administration, the DLW can be sterilized by pushing it through a 0.22 μm filter.
Calculation of AEE and physical activity level (PAL)
After its measurement by the DLW method, TEE can be used for the calculation of AEE and PAL. The calculations involve REE, which is measured by indirect calorimetry [37] or estimated by using predictive equations [38]. With the TEF assumed as 10% of TEE, the AEE is calculated as follow [6]:
The following equation is used for the calculation of PAL:
DIRECT CALORIMETRY
The direct calorimetry technique measures the rate of heat loss by the subject using a calorimeter. It is the most accurate method for quantifying metabolic rate [39], but its use is limited by the high cost. There are 4 types of direct calorimeters, namely the “isothermal direct calorimeters” (also known as “heat-flow or heat-conduction calorimeters”) [40] which work by maintaining a constant wall temperature by means of a constant temperature fluid (commonly water) in a jacket or bath surrounding the animal chamber, or in a network of copper tubing bonded to an exterior wall surface; the “heat sink direct calorimeters” which are made of a chamber from which heat lost by the subject is removed by a liquid-cooled heat exchanger [41]; the “direct convection calorimeters” which consist of an insulated chamber ventilated with an air flow at a known rate. The system works by determining the temperature and enthalpy differences between the air entering and exiting an insulated chamber [4243]; and the “direct differential calorimeters” which involve 2 identical chambers, one housing the subject and the other having an electric heater adjusted to yield identical temperature increases in both chambers [39].
INDIRECT CALORIMETRY
The technique of indirect calorimetry relies on the measurement of inspired and expired gas volume, and the concentrations of O2 and CO2 [37]. Various methods are used for gas collection, including the Douglas Bag [44], the canopy [45], and the face mask [3746]. Indirect calorimetry is an accurate and noninvasive method, and it can allow the assessment of energy expenditure on field through the use of ambulatory metabolic systems [47]. Energy expenditure is calculated by Weir's formula [48] which is as follow:
where VO2 is the volume of consumed O2 and VCO2 is the volume of produced CO2.
where VO2 is the volume of consumed O2 and VCO2 is the volume of produced CO2.
Indirect calorimetry is the most widely used method to assess energy balance, including those involving patients in clinical setting [5051]. In other studies, it has served as a reference method to assess the accuracy of other methods of energy expenditure measurement, such as the validation of accelerometers [52] or predictive equations for REE [5354]. In comparison to the direct calorimetry, the method is more affordable, and presents the advantage of providing information on the metabolic fuels being combusted in addition to measuring the metabolic rate [39].
ACCELEROMETRY
Recent advances in technology have permitted the development of accelerometers as one of the methods of physical activity energy and expenditure measurement. These tools have proven to be reliable, objective, less burdening to participants, versatile and less costly compared to other methods of physical activity energy estimation [55]. Today, different models of accelerometers have been developed by different companies, and are available on the market. Their detailed specifications have been described elsewhere [56]. For the Actigraph accelerometer and Actical accelerometer models, different generations have been developed over time as described in a study by John and Freedson [57].
This method is based on measurement of the body's acceleration, which is the change of velocity over time and is expressed in terms of multiples of gravitational force (g = 9.8 m/S2) [6]. Certain models measure acceleration in 1 plane (uniaxial), 2 planes (biaxial), or 3 planes (triaxial accelerometers). Accelerometers generate their output in form of “counts” per unit time. To convert these counts in energy expenditure units, predictive equations have been developed. Some of equations permit to calculate energy expenditure as metabolic equivalents (METs) [585960] or kcal/min [6061]. Validation studies for these equations have been conducted using indirect calorimetry [52] or the DLW method [2362]. In a recent study, Lyden et al. [63] evaluated the accuracy of commonly used accelerometer equations for the prediction of energy expenditure and METs. Their findings indicated that current accelerometer prediction equations have many limitations when translating accelerometer counts to energy expenditure, especially when used across a range of various activities.
The first Actigraph models developed are uniaxial accelerometer [60] and recently, new models have been developed which measure acceleration in 3 planes (triaxial accelerometers) [64]. In these latter models, energy expenditure can be calculated by integration of counts from the 3 planes, namely the vertical (Y), the horizontal right-left (X) and the horizontal front-back axis (Z) [64]. In this case, energy expenditure is predicted by what is known as vector magnitude (VM).

Where X, Y, and Z are the sum of counts from X-axis, Y-axis, and Z-axis, respectively.
One of the questions that have been raised with the development of new generations of accelerometers is the comparability between their output and the previous generations. It has been shown that there is comparability between uniaxial and triaxial generations of the same accelerometer model when counts from the vertical axis are used, but this is not applicable in case the VM counts from the triaxial accelerometer are used [65].
HEART RATE MONITOR
Heart rate monitors are among commonly used objective tools for measuring physical activity and energy expenditure [6667]. Their use is based on the assumed relationship among heart rate, activity intensity and oxygen consumption since physical activity puts the heart under pressure to deliver more oxygen to exercising muscle cells [68]. Studies have established that heart rate changes proportionally with activity intensity and oxygen consumption in moderate to vigorous physical activities [69]. However, this correlation is low in case of sedentary and light activities, and it remains one of the limitations of heart rate monitors [687071]. The relationship between heart rate and VO2 is affected by confounding factors such as specific muscle mass utilization, type of activity, physical fitness levels, and other exercise-related factors [6]. Some non-exercise factors have also been reported to affect the relationship between heart rate and VO2. Studies have reported electrical or magnetic interference with the heart rate measurements by devices such as computers, microwaves, televisions, and motorized exercise equipment, leading to unstable readings and data loss [72]. Suggestions to reduce this problem of electrical interference include keeping the heart rate monitor at least 1 meter away from the electrical circuit of electrical devices, and to position the heart rate receiver close to the transmitter, thus strengthening the transmitter signal relative to the interference signal [6].
Despite these limitations, heart rate monitors remain popular among researchers as they present advantages of relatively low cost, noninvasive nature and versatility. Their use provides the objective and reliable information on energy expenditure and intensity and duration of activity [697374]. Different studies have shown validity of these tools in controlled settings [6975] as well as in free living conditions [7677].
PEDOMETRY
Pedometers are used in the measurement of walking, which is one of the most frequently performed activities and contributes a large proportion of physical AEE on physical activity questionnaires and logs [6]. The basic output of pedometers is in form of step counts. In addition to this, it is possible to use pedometers for estimating the distance traveled by multiplying the number of steps by stride length. Stride length is affected by factors including walking speed, height, age, and gender [78]. Some pedometers display energy expenditure as kilocalorie [79], but it is not clear whether they display gross or net kilocalories. Crouter et al. [79] assessed the validity of 10 electronic pedometers for measuring steps, distance, and energy cost, and found that these tools are the most accurate for assessing steps, less accurate for assessing distance, and even less accurate for assessing kilocalories. In spite of their low accuracy, pedometers have an advantage of low cost, and they can be used as self-monitoring tools for people who want to maintain their PAL [8081].
SELF-REPORT METHODS
The most widely used self-report methods for assessment of physical activities include methods such as physical activity questionnaires and physical activity records and diaries. They have been used in large cohort studies, which have allowed establishing the protective role of physical activity against diseases including metabolic syndrome-related disorders (insulin resistance, type 2 diabetes, dyslipidemia, hypertension, and obesity), heart and pulmonary diseases (chronic obstructive pulmonary disease, coronary heart disease, chronic heart failure, and intermittent claudication), muscle, bone and joint diseases (osteoarthritis, rheumatoid arthritis, osteoporosis, fibromyalgia, and chronic fatigue syndrome), cancer, depression, asthma and type 1 diabetes [82]. The limitation of these self-report methods of physical activity assessment is their low accuracy and reliability [83], as shown by various validation studies using objective measures of physical activity or energy expenditure such as the DLW method [84] and accelerometers [8586]. Nevertheless, they are more affordable due to low cost compared to other method of physical activity assessment. They provide information concerning the participants' physical activity patterns [6].
The most commonly used physical activity questionnaires include the International Physical Activity Questionnaire (IPAQ) [8788], the 7-day Physical Activity Recall (PAR) [30], the Modifiable Activity Questionnaire (MAQ) [89], the Previous Week Modifiable Activity Questionnaire (PWMAQ) [90], the Recent Physical Activity Questionnaire (RPAQ) [91], and the Previous Day Physical Activity Recall (PDPAR) [92]. Details on these questionnaires are provided elsewhere [93]. These questionnaires present a low burden to subjects, but they are limited by their relying on the participant's memory of performed physical activities, increasing the risk of memory bias [6]. Since physical activity records and diaries require participants to record performed activities, they minimize the memory bias in case they are completed on time. However, the burden to participants is higher compared to physical activity questionnaires and the delay to record may lead to memory bias and reactivity [93].
CONCLUSION
In summary, there is no single best method that can assess all aspects of physical activity and energy expenditure. Therefore, as suggested by Troiano [94], the choice of assessment instrument depends on what aspect of physical activity the researcher wants to measure, characteristics of the target population, and whether the data will be used to describe groups or individuals.
 XML Download
XML Download