

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obesity is referred to as a serious health problem worldwide, shortening life, and threatening the quality of life [1]. The prevalence of adult obesity in Korea increased from 26.0% in 1998 to 31.7% in 2007 and remained at 33.2% in 2015 [23]. In addition, the prevalence of morbidly obese (MO) with body mass index (BMI) of 30 kg/m2 or more was 3.1% in male and 3.6% in female over 20 years of age in 2010 compared with 1998, which is more than double [45]. According to the Korea National Health and Nutrition Examination Survey, the risk of complications such as hypertension, diabetes mellitus, and dyslipidemia was more than 2 times higher in obese people than people in normal weight [6].
In particular, type 2 diabetes mellitus (T2DM) has a higher relative risk of obesity than hypertension or other obesity complications [7]. It has been reported that visfatin secreted from visceral adipocyte, is closely related to the induction of complications of T2DM by directly contributing to insulin resistance [8]. Kenkel and Manning [9] reported that 60% of diabetic patients were associated with obesity, while Colditz [10] reported that about 57% of diabetic patients were associated with obesity. In Korea, the relative risk of T2DM was higher in the obese group than in the non-obese group [11]. The prevalence of T2DM in adults over 30 years of age has remained at around 9% since 2005, with 9.5% in 2015. The mortality rate from diabetes mellitus was 24.0% in 2005 and 20.7% in 2015 [23].
Methods for treating obesity include surgical and non-surgical methods such as diet, exercise, behavioral therapy, and medication [13]. The bariatric surgery methods include adjustable gastric banding, laparoscopic adjustable gastric banding (LAGB), sleeve gastrectomy, Roux-en-Y gastric bypass (RYGB). Bariatric surgery has been used as a treatment for obesity in the US and has increased 9-fold from 13,386 in 1998 to 121,055 in 2007 [11]. In Korea, the rate of bariatric surgery increased sharply from 139 in 2003 to 1,687 in 2013 [14]. Many studies have reported that bariatric surgery is effective not only for obesity, but also for diabetes treatment [15]. Improvement of T2DM has been reported after sleeve gastrectomy for the treatment of MO patients [16]. In addition, in cases of MO diabetic patients, the bariatric surgery group showed improvement in physical health and quality of life compared with the non-surgery group [12]. However, the studies on LAGB surgery have been limited to studies on obesity treatment, and studies on the effect of LAGB surgery in morbid obese diabetic on diabetes improvement have been lacking in Korea [1718]. Therefore, in this study, we investigate the effect of LAGB surgery on the improvement of MO patients with T2DM.
MATERIALS AND METHODS
Subjects
This was a retrospective study, using patients' medical records at C surgical hospital in Seoul. We analyzed data from MO patients who received LAGB surgery with or without T2DM. The study included data collected during April 2014 to March 2016. The subjects' medical records included information on sex, age, height, weight, body composition, blood pressure, and blood metabolic profiles. Changwon National University's Institutional Review Board (IRB) approved this retrospective medical record review (IRB No. 104027-201604-HR-006). We analyzed their medical record before LAGB and a year after LAGB. Subjects whose BMI were less than 30 kg/m2, under 18 years of age and absent medical record before and after LAGB were excluded from the study. The participants were divided into 2 groups according to their glycated hemoglobin (HbA1c) levels. The number of total subjects included was 88; of whom 38 with high HbA1c levels (> 6.5%) were in the MO with T2DM (MOD) group and 50 subjects with HbA1c less than 6.5% were in the MO group.
Anthropometric analysis
For all the subjects, anthropometric measurements were measured. Height and weight were recorded to the nearest 0.1 cm and 0.1 kg using an automatic height-weight scale. BMI was calculated by dividing weight (kg) by height squared (m2). Percent body fat, lean body mass, body water, obesity degree, and visceral fat area were measured by bioimpedance analysis (Inbody 3.0; Biospace, Seoul, Korea). Waist and hip circumference were measured with a flexible measuring tape. Waist circumference was measured between the costal inferior border and the iliac crest. Hip circumference was measured at the widest point of the hip.
Biochemical analysis
All blood samples were sent to the Green Cross Laboratory (Yongin, Korea) for analysis. The analysis of HbA1c, hemoglobin (Hb), hematocrit (Ht), albumin, triglyceride (TG), total cholesterol (TC), aspartate transaminase (AST), and alanine transaminase (ALT) were commissioned.
Statistical analysis
Statistical analyses were performed using SPSS software version 21.0 (IBM SPSS Statistics for Windows; IBM Corp., Armonk, NY, USA). Measurement data were presented as mean ± standard deviation (SD). The difference between the MOD and MO groups was analyzed using t-test. The values for pre-operation and a year after operation were compared using paired t-test. In addition, categorical data were compared using the χ2 test. All statistical results were verified with the significance level set at p < 0.05.
RESULTS
General characteristics
General characteristics of the MOD and MO groups are summarized in Table 1. In the MOD group, 5 males and 33 females participated; and in the MO group, 6 males and 44 females participated. There were no differences between the 2 groups in weight, height, BMI, and blood pressure. However, severe obese patients with a BMI over 40 in the MOD group were more than those in the MO group. In the MOD group, 10 and 12 subjects had hyperlipidemia and hypertension, respectively; and in the MO group, 6 and 4 subjects had hyperlipidemia and hypertension, respectively. Thus, patients with hyperlipidemia and hypertension were more frequently found in the MOD group.
Table 1
General characteristics in MOD and MO patients

Values are presented as number (%) or mean ± standard deviation. Analyzed using t-test for continuous variables and χ2 test for categorical variables between the groups (MOD vs. MO).
MOD, morbidly obese patients with diabetes; MO, morbidly obese; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure.
![]()
Changes in anthropometric indices after gastric banding surgery
Anthropometrics parameters are presented in Table 2. The result of anthropometrics indices before and after surgery showed significant reduction of body weight, BMI, body fat, fat-free mass (FFM), waist/hip ratio, visceral fat area, and obesity degree in the MOD and MO groups (p < 0.001). Especially, the decrease rate of the visceral fat area was the highest among the anthropometric measurement both in the MOD and MO groups (−36.3% ± 24.6% and −46.9% ± 25.3%, respectively). The changes in anthropometric indices of MO group before and after surgery were higher than those of MOD group, but there was no significant difference between the 2 groups.
Table 2
The changes of anthropometric parameters in MOD and MO patients after gastric banding surgery

Values are mean ± standard deviation.
MOD, morbidly obese patients with diabetes; MO, morbidly obese; T0, at baseline; T1, after gastric banding surgery; BMI, body mass index; FFM, fat-free mass; Vfat, visceral fat area.
*T0 vs. T1 by t-test.
![]()
Changes in metabolic profiles after gastric banding surgery
Blood biochemical analyses before and after LAGB are presented in Table 3. The results showed that the levels of AST, ALT, and HbA1c had significant reduction in each group. Although AST and ALT, as indicators of liver function, were higher than normal range prior to surgery, it was within normal range after the surgery in both groups and thus it was shown that the surgery was also effective in the treatment of fatty liver. For HbA1c, treatment rate was 71% in the MO group with T2DM with significant reduction of 22.8%, and there were 6.1% of significant reduction in general MO patients. It was found in this study that the reduction of HbA1c was greater as the pre-operative early body weight was heavier.
Table 3
The changes of biochemical parameters in MOD and MO patients after gastric banding surgery

Values are mean ± standard deviation.
MOD, morbidly obese patients with diabetes; MO, morbidly obese; T0, at baseline; T1, after gastric banding surgery; Hb, hemoglobin; Ht, hematocrit; TG, triglycerides; TC, total cholesterol; AST, aspartate transaminase; ALT, alanine transaminase; HbA1c, glycated hemoglobin.
*T0 vs. T1 by t-test.
![]()
The ratio of changes in metabolic profiles after surgery is shown in Figure 1. The levels of TG and TC were not significantly change after LAGB of the MOD (−39.3% ± 33.4% and −2.9% ± 27.0%, respectively) and MO (−29.7% ± 38.4% and −2.3% ± 21.9%, respectively) groups. There were no significant differences in AST and ALT levels in the MOD (−19.7% ± 53.2% and −53.4% ± 31.0%, respectively) and MO (−26.6% ± 40.5% and −48.6% ± 32.8%, respectively) groups. LAGB surgery significantly lowered HbA1c levels in the MOD group (−22.8% ± 10.5%) compared with those in the MO group (−6.1% ± 6.7%, p < 0.05).
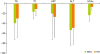 | Figure 1The ratio of changes of biochemical parameters in MOD and MO patients.
MOD, morbidly obese patients with diabetes; MO, morbidly obese; TG, triglycerides; TC, total cholesterol; AST, aspartate transaminase; ALT, alanine transaminase; HbA1c, glycated hemoglobin.
*Significantly different between the values at MOD and MO groups by paired t-test (p < 0.05).
|
DISCUSSION
This study investigated the effect of LAGB surgery on the improvement of HbA1c of MO patients with T2DM with the consideration that obesity was associated with insulin resistance and T2DM. This is a retrospective study using the medical records of pre- and post-operative 38 MO patients with T2DM and 50 MO patients among patients who have undergone LAGB.
A total of 88 patients were selected as the study subjects, and analysis was performed by classifying people with ≥ 6.5% of HbA1c as the group of MOD and people with < 6.5% as the group of MO in reference of HbA1c of 6.5%. In this study, the mean age, weight, and BMI were 34.3 ± 8.9 years, 99.9 ± 21.1 kg, and 37.3 ± 7.4 kg/m2, respectively, which was similar to those of Kim et al. [13]. In the present study, there were no significant differences in pre-operative anthropometric data between the 2 groups. Schindler et al.'s study [17], in the obesity study, the mean weight of the subjects was 127.5 ± 4.1 kg and the mean BMI was 44.8 ± 1.0 kg/m2. In Giusti et al.'s study [18], the mean weight of the subjects was 118.6 ± 14.5 kg and BMI was 43.6 kg/m2. These results indicate that the standard of BMI for obesity, according to the World Health Organization (WHO) criteria, is lower in Korea than in Western countries [19]. Our study showed that body weight, body fat, FFM, waist/hip ratio, and visceral fat area decreased after LAGB compared to pre-operation (Table 2). Body weight decreased from 102.9 ± 19.2 kg to 82.5 ± 18.6 kg in the MOD group, and decreased from 97.4 ± 21.8 kg to 73.7 ± 18.6 kg in the MO group. Patients in both groups showed significant decreases in their body weight as compared to the pre-operation. BMI decreased significantly from 38.1 ± 6.1 kg/m2 to 30.6 ± 5.9 kg/m2 and from 27.6 ± 6.3 kg/m2 to 36.6 ± 8.0 kg/m2, in the MOD and MO group, respectively. Therefore, it was found that weight loss continued after surgery. This decrease in body weight and BMI was similar to that of RYGB reported by Kim et al. [13]. In addition, the rate of change for visceral fat area in the MOD and MO group significantly decreased compared to pre-operation (−36.3% ± 24.6% and −46.9% ± 25.3%, respectively). Visceral fat obesity was defined by obese subjects with visceral-subcutaneous fat ratio (V/S ratio) of ≥ 0.4, whereas obese subjects with V/S ratio of < 0.4 were defined as subcutaneous fat obesity [20]. Visceral fat is one of the predictors of cardiovascular disease (CVD). Also, visceral fat obesity is thought to be a basic pathology for metabolic syndrome (MS) [21]. We also found that the LAGB caused decrease in body fat mass of the MOD and MO groups. These findings are in line with previous studies demonstrating that LAGB decreased body fat mass [18]. This is similar to the decrease rate in body fat mass 27.3% in Giusti et al. [18]. However, Carey et al. [22], significant decreases in body weight (−50.9 kg) and body fat mass (−75.2%) were observed from pre-surgery to post-bariatric surgery. Carey et al.'s study [22] showed that the body fat reduction rate was higher than that in our study, but this result may be due to the difference according to the operation method. These results demonstrate that LAGB decreased body fat mass, body weight, and the risk of obesity related complications in MO patients with or without T2DM.
In this study, LAGB significantly reduced the HbA1c level from 8.3% ± 1.9% to 6.4% ± 1.5% in the obese diabetic patients. Among the total T2DM, 71% of subjects (21 patients) showed decrease in HbA1c less than 6.5%. Swedish obese subject (SOS)'s study [23], Buchwald et al. [24], and Pories et al. [25] reported that bariatric surgery is effective in diabetes treatment. Also, there was a difference in treatment rate between 45% and 100%, depending on the type of surgery. HbA1c is an important bio-marker for long-term glycemic control and reflects fasting blood glucose and postprandial glucose. HbA1c is a better predictor of diabetic complications than fasting glucose [2627]. These results suggest that reduction of HbA1c in response to LAGB could contribute to decreasing risk of diabetic complications [28]. The bariatric surgery is effective in treating T2DM because of weight loss. Weight loss is very important in the treatment of diabetes and it is known that 10% reduction in body weight reduces the incidence of diabetes by more than 50% and reduces diabetes-related mortality by 20% [29]. In the present study, the MOD group showed average of 19.6% weight reduction after LAGB, suggesting that diabetes treatment was effective. Also, these results suggest that the higher body weight before the weight loss was associated with the greater reduction rate of HbA1c and the effect of diabetes treatment. In the study, LAGB was more effective in decreasing HbA1c in the MOD group, suggesting that LAGB improved hyperglycemia and T2DM.
Hyperlipidemia was also present in the obese patients with or without T2DM, and the TG levels were also decreased to normal level after LAGB. The decrease of serum TG levels was thought to be due to the decrease of calorie intake after LAGB. Also, these results are similar to Kim et al.'s report [13]. It is known that the majority of obese patients have fatty livers [30]. As a result, this study also showed that serum ALT and AST levels exceeded the normal range in both groups, indicating the problems in liver function. The MOD and MO groups showed the normal range of serum ALT and AST levels after LAGB. Significant reductions in serum ALT and AST levels were similar to those of Mummadi et al.'s report [31]. Also, serum ALT levels showed greater changes than serum AST levels. After the gastric band surgery, changes in HbA1c and liver function indicators showed improvement not only in T2DM but also in fatty liver.
Through this study, it was found that LAGB had therapeutic effect in MOD patients. It is thought that bariatric surgery is one of the breakthrough methods not only for weight loss but also for the prevention of complication, including diabetes mellitus in obese patients. Although LAGB has less beneficial effects compared to other bariatric surgeries, it is relatively simple and safe, and thus there would be substantial demand in the treatment of MOD in the future. As the study about bariatric surgery mostly focuses on weight loss, there is lacking in study about surgical effect of MOD.
However, there are some limitations in this study. This was a retrospective study, using restricted medical records. Thus, there was no data on fasting blood glucose, glucose tolerance test, or insulin tolerance test. In the future, study about bariatric surgery in MOD and the study comparing the effects in MOD according to the type of surgery would be necessary. Also, studies investigating other effects of surgical complications of morbid obesity would be required.
In conclusion, LAGB alleviated T2DM in MOD group, in part by improving HbA1c levels. Thus, LAGB may be useful for improving overall glycemic control in the management of DM in MOD patients.
 XML Download
XML Download