

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Breast cancer (BC) is the main common cause of cancer mortality among women in the world [1]. Age, and family history are the most critical BC risk factors [23]. Among Palestinian women, it is 30.6 percent of women's cancer and the incident rate is 78.9 per 100,000 women in 2014 and increased to 83.9 per 100,000 in 2015 [45]. However, few studies have tackled the risk factors of BC in Palestine [6]. The problem of BC is noticeably growing in developed and developing countries. In various regions, BC is the most frequently occurring malignant disease among women and comprises 18% of all female cancer [7]. Annually, a million—new case of female BC are diagnosed worldwide, most of them are in developed countries [8].
BC is cancer that starts in the cells of the breast in women and men. Generally, it refers to a malignancy in women that arises from the terminal ductal-lobular units of epithelial tissue, which represent 10% of the total volume in the mature breast [9]. The proportion of BC in Palestine is like that in the neighbouring countries unlike to those in Lebanon, as BC accounts for nearly half of all cancers among Lebanese women [10]. According to the preliminary interview with the director of women health department doctor Sawsan Hammad, BC available services in Gaza Strip are 20 mammogram machines distributed all over Gaza governorates. In this regard, 5 mammogram machines are in governmental service as 4 are functioning and the 5th is out of order. The remaining 15 mammogram machines are in the private and non-governmental organization. She added that Ministry of Health (MOH) services are for free. However, in the private services, the screening mammogram must be paid, as patients pay from 10–15 USD. Due to certain factors such as; high total fertility rate (4.6%), high rate of breastfeeding (95.6%) with a mean duration of 10.9 months, young mean age at first birth (20 years), and no alcohol consumption, the Palestinian women are protected against BC [6]. However, reports from MOH and other studies concerning the Palestinian community have shown an increase incidence of BC [4]. Moreover, there are limited studies and insufficient knowledge about this disease in the developing countries. It is worth mentioning that risk factors are associated with the development of BC were not studied before among the women in Gaza after the war 2014.
This study aimed at exploring the various risk factors associated with the development of BC in women in the Gaza Strip, Palestine. This study may help to understand the interaction of these factors that find a way for cancer development among the Palestinian women in order to set guidelines for prevention strategies of BC in Palestine.
MATERIALS AND METHODS
The hospital-based case-control study collected information on women residing in the Gaza Strip, as the age of the enrolled cases and controlled ranged between 18 to 60 years old. Geographical location and age were matched for both the case and control groups (with an interval of ± 3 years). The data of the cases of this study was collected in the Department of Oncology at Al-Shifa Hospital in the Gaza City and the European hospital, over the period of October 2014 to February 2015.
The selected cases were recorded and confirmed during the period beyond 2014 in cooperation with cancer registry centre to revise documents of the patients. Face-to-face interview was conducted during the patient visit to the oncology department.
A hospital-based group matched case-control study was conducted to identify BC risk factors. The study tackled of 105 hospitalized cases confirmed on histopathology and 209 group-matched controls selected from same geographical area without history of breast problems or neoplastic disease and not had any other cancers. Two controls from the neighbours of these cases were visited at home to be studied. Written approval was obtained from the MOH to access the patients' records from the oncology department and cancer registry. Meanwhile, written consent form was obtained from the study sample.
Different risk factors (independent variables) that may interfere in BC were studied. A structured questionnaire included; the status of education, menstruation cycle, the induced abortion history, first-degree family history of BC, parity, number of full-term pregnancies, duration of breastfeeding (month), age at first pregnancy (year), age at menarche, history of irregular menstruation, spontaneous abortion, history, duration of using oral contraceptives, benign breast disease personal history, smoking, body mass index (BMI), hypertension (HT), and diabetes.
Anthropometric measurements, with 2 variables height and weight were used. Body weight of each participant was measured by using a calibrated scale (Seca model 750 1017009; Seca GmbH, Hamburg, Germany). Participants were weighed barefooted to the nearest 0.5 kg. Using the stadiometer (Seca body meter 206; Seca GmbH), height was approximated to the nearest 0.5 cm without shoes, the shoulders in a relaxed position, and the arms hanging freely. A single derived variable BMI was used in this study.
SPSS version 21 (IBM Corp., Chicago, IL, USA) was used for the data analysis, as bivariate and multivariate conditional logistic regression was used to assess the association of BC with independent variables and crude and adjusted odds ratio (OR) and related 95% confidence intervals (CIs) were calculated to determine the precision of the estimates. The level of significance used was 5%. The p value < 0.05 indicated significance.
RESULTS
The distribution of patients with BC (n = 105) and control (n = 209), according to socio-demographic characteristics (age, governorates, resident, locality of residence, and home type) is shown in Table 1. The age of the majority of the study sample was above 40, while the majority of them were city inhabitants.
Table 1
Study population distribution according to the socio-demographic factors
According to BMI, marital status, age at marriage and education, the distribution of patients with BC (n = 105) and control (n = 209) as shown in Table 2. The BMI ≥ 30 kg/m2 was reported among 58.3% of the cases and among 30.5% of the control. Regarding marriage age, i.e., less 19 years old, 42.7% was among the cases while 35.9% among the control.
Table 2
Study population women distribution according to the social status and BMI
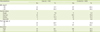
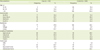
Table 3 shows the distribution of the study population according to some reproductive health factors. Regarding the age of menarche, the table shows that double percent among the cases have menstruation before the age of 11 compared to the control. It also shows that women with more than 5 children and those of null parlous are more among the cases compared to the control.
Table 3
Study population women distribution according to the reproductive health factors, passive smoking, examination of breast, and other factors
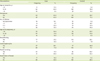
Table 4 shows the distribution of study population according to the family history and some chronic diseases that are common in the Gaza Strip. The table shows that 81.6% were first-degree relatives of BC patients among the cases, while 61.9% were among the control. The same table shows that 24.8% and 21.0% were diabetes and hypertensive among the cases, while 6.2% and 7.7% among the control.
Table 4
The control and case groups regarding medical history factors

Table 5 shows the risk factors that increased BC, as women that had a late pregnancy (> 35 years) (OR, 11.56; 95% CI, 1.64–81.35) and those with BMI (≥ 30 kg/m2) (OR, 4.70; 95% CI, 1.62–13.69). It also shows that first-degree family history of BC (OR, 2.7; 95% CI, 1.04–7.20), while hypertensive patients (OR, 12.13; 95% CI, 1.93–76.10), and those with diabetes mellitus (DM) (OR, 6.84; 95% CI, 1.77–26.36).
Table 5
Risk factors associated with increased or decreased risk of BC

DISCUSSION
The findings of this study have revealed several risk factors for BC among women living in the Gaza Strip. These factors were found to be associated with increased BC risk including late pregnancy (> 35 years), high BMI, first-degree relative history, HT, and diabetes. While there was no reported statistical association concerning the place of living, exposure to passive smoking or even being breastfed. On the other hand, several factors seemed to be protective factors for BC including null parity, women with more than 5 children, and the age at first menstrual period “menarche.”
Wide ranging investigations have uncovered that when compared to women without a family history of BC, women with a first-degree relative (mother or sister) diagnosed with BC face almost twice the possibility of contracting this ailment. This possibility is aggravated in a situation where the number of relatives stricken with BC is two or more [11]. It is fairly accurate to surmise that in developed countries, 25% of inter-individual differences linked to BC exposure is attributed to genetic issues, while the remaining 75% is attributed to issues concerning the individual's surroundings and way of life [12].
The present study revealed a relationship with statistical significant between BC and the family history. This familial association for women in Gaza is likely to imply a genetic predisposition. Therefore, it is of interest to investigate more about this association to determine the responsible gene.
A different conclusion has been observed regarding the exposure to passive smoking, using the contraceptive pills and practising of breastfeeding with the incidence of BC, as there were no statistically significant relationships.
According to results derived from investigations on several ethnic groups, the threat of BC is elevated during an older woman's first full-term pregnancy [13141516]. In contrast, other studies revealed different results which were inconsistent with our findings [1718].
This study puts forward that pregnancy during an advanced age (35 years and more) can encourage the progress of existing malignancy cells. Pregnancy brings about terminal differentiation of human breast glands which may have a less pronounced proliferative element. The initial pregnancy stimulates permanent alterations that either reduce the vulnerability of the breast tissue to the occurrence of cancer, or decrease the carcinogenic stimulus to the breast [19].
A separate threat related to the development of BC is BMI. According to results attained from our investigations, women with a BMI in excess of 30 kg/m2 are more susceptible to BC than women with a BMI lower than 30 kg/m2. This revelation is in agreement with results acquired through previous studies [202122]. The link between obesity and BC can be traced to the abundance of body fat accumulation. This situation, which contributes to the peripheral conversion of lipocytes into oestrogen, encourages the development of cancer cells. Another factor that requires consideration is excessive insulin. As insulin fuels the development of BC cell lines, its raised levels in obese women can heighten the threat of BC. Peptides that contribute towards the regulation of tissue development and fat deposition are known as insulin-like growth factors (IGFs). IGF-1 is an insulin-like growth factor that sets off mitosis in BC cells. Several epidemiologic investigations have revealed that the levels of IGF-1 may be elevated in women who are obese. This circumstance exposes them to a higher risk of developing BC [20]. From a chemical standpoint, the raised risk of BC in obese women can generally be put down to the alteration of androstenedione into adipose tissue (the main supplier of oestrogen in post-menopausal women). An outsized amount of adipose tissue leads to the development of an estrone level that is proportionate to this amount [23].
Findings of the present study also indicated a positive correlation between diabetes (type II diabetes) and BC. The result was consistent with another case-control and cohort study carried out in North America, Europe, and Asia [24]. Palestinian health reports indicated that chronic diseases like HT and diabetes are rising in Palestine. The increase of chronic diseases epidemics are propelled by social, economic, and demographic factors, of which urbanisation and globalisation are the main determinants [25]. The mechanisms underlying the relationship between diabetes and BC risk may be related to alterations in circulating concentrations of insulin, IGFs and endogenous sex hormones. Diabetes type II is usually combined with insulin resistance and increased pancreatic insulin secretion for long periods before and after disease onset. Insulin has been demonstrated to have mitogenic effects on breast tissue and insulin receptors are frequently over-expressed in BC cells. A positive association between circulating concentrations of insulin or C-peptide (a marker of insulin secretion) and BC risk has been observed in another epidemiologic study [24]. More in-depth investigations are needed to identify the relationship especially with the higher prevalence of DM in Gaza Strip.
No doubt that HT is a main cause of mortality and morbidity, especially prevalent in the developed world. The relationship between HT and BC is controversial. Some studies report a weak-to-moderate association between HT and BC in menopausal women [26272829], but this finding is not consistent with other studies [30313233]. Some researchers concluded observed association between HT and BC is confounded by obesity and high BMI, which is a risk factor for both BC and HT [3435]. In the present study, HT is recorded as one of the main BC risk factors. Further investigations are needed to figure out whether HT, obesity, high BMI, or the drugs used for the treatment of HT are responsible for increasing the risk of BC. While other reproductive factors in this study are well established as risk factors for BC, while the rest reproductive factors were reported as protective factors of BC.
The results indicated that higher numbers of births are recognised as protective against BC. The present data provide evidence that, among nulliparous women, a high number of births (≥ 5 births) are associated with decreased BC risk in the target group of the study. Several researchers reported that the degree of BC risk faced by women who have delivered five or more children is half that of women who have not experienced labour and delivery [36]. However, other investigations disclosed that the decreased risk factor related to the raised number of births may be confined to hormone receptor-positive BC [37]. Then again, this finding is contradictory to that obtained through a different investigation [38].
The nulliparity of some women in the BC group can be put down to their non-married status or infertility. A significant number of researchers are convinced that nulliparous women face a greater risk of coming down with BC [394041]. A study involving Norwegian women indicated that nulliparity and obesity can exert a synergistic influence on the BC risk of more mature women [42]. Contrastingly, the results from our investigations signify that instead of raising the risk of BC in women, nulliparity fortifies the protection against this disorder. Garland et al. [43] discovered that due to their lesser exposure to ovulatory cycles, women beset with ovulatory infertility are less vulnerable to BC. It was also uncovered that clomiphene citrate, an ovulation-stimulating agent and oestrogen adversary resembling tamoxifen, is linked to the reduced BC risk in women who are incapable of conceiving due to infertility.
Early age at menarche is a known risk factor for BC. In the present study, women who had menarche at age 13–15 years old were at decreased risk compared with women who had menarche at an early age less than 13 year. Menarche at the age of 13–15 years was associated with decreased risk of BC and the difference was statistically significant (p = 0.026). This finding was matched with other studies from Saudi Arabia, Cyprus, and Japan [684445]. Female with a menarcheal age, below 12 years, had higher serum estradiol but lower testosterone and dehydroepiandrosterone concentrations, compared to those with later menarche [46].
CONCLUSION
The strongest associations with BC risk Palestinian women population were observed with late age a full-term pregnancy, high BMI and first-degree family history of BC. Overall, the findings of current study corroborate with the results of previous investigations on descriptive epidemiology of risk factors for BC. However, the current study presents the first publication for BC risk factors among women in Gaza after war 2014 in Gaza and provides the first scientific evidence using local data, for executing more targeted campaigns of prevention and early diagnosis among Palestinian women population. More in-depth investigations are needed to identify the relation especially with the higher prevalence of BC in Gaza Strip, Palestine.
 XML Download
XML Download