

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The metabolic syndrome (MetS) is a cluster of metabolic risk factors that can lead to chronic diseases [1]. Although the history of MetS is back to many years ago, but the modern era of that has started with description by Reaven in 1980 [2]. The National Cholesterol Education Panel-Adult Treatment Panel III (NCEP-ATPIII) defined MetS by the presence of obesity, dyslipidemia, elevation of arterial blood pressure and glucose intolerance [3].
This syndrome can increase the risk of cardiovascular disease (CVD), diabetes mellitus, stroke, and even cancers [456]. Based on these reports, the prevalence of MetS is variable in worldwide and Iranian community [78] and relatively high in different area of Iran(more than 25%) [910]. The etiology of MetS has not been revealed elearly. However, it is proposed that genetic, metabolic and environmental factors play important roles in this [1112].
Although the complementary therapies existed many years ago around the world, but the standard herbal medicine has started in recent decade and is considered as new approach to preventing and curing of diseases such as MetS, diabetes mellitus, and CVD [13]. Nowadays, there are much more attention to use of plants as therapeutics, because of lower adverse effects of Nigella sativa (N. sativa) or Black seed that belongs to family of Ranunculaceae has been used to improve health and cure diseases for centuries especially in the Middle East and Southeast Asia [14]. A great focus is done on several traditional uses and therapeutic properties of N. sativa [15]. The therapeutic properties of N. sativa is attributed to several components including proteins, amino acids, carbohydrates, fibers, oils (combination of fatty acids especially polyunsaturated fatty acids), volatile oil (frequently thymoquinone), mineral, alkaloids, flavonoids, saponins, and so on [16].
Effects of supplementation of N. sativa is evaluated on blood parameters in several studies. Lipid profiles include triglycerides (TG), cholesterol (CHOL), low density lipoprotein (LDL-CHOL), high density lipoprotein (HDL-CHOL), and also LDL/HDL-CHOL are important metabolic indices in many diseases such as MetS. The effects of supplementation of N. sativa on lipid profiles have been controversial in MetS as these effects in some of studies have been significant but not in others [1718]. The effect of N. sativa on inflammatory factors such as C-reactive protein (CRP) is also evaluated in few studies but results were not the same. In a study, N. sativa supplementation reduced serum CRP in patients with coronary artery diseases [19] but this effect was not significant on high-sensitivity CRP (hs-CRP) in subjects with obesity [20]. Apolipoproteins (Apos) are useful indicators in evaluation of blood lipid status in human. The level of Apo-A correlates with HDL-cholesterol and Apo-B with LDL-cholesterol. These indices give us accurate information about features of lipid disorders, but there is no evidence about effects of N. sativa on apolipoproteins.
Because the pharmacological forms of N. sativa supplementation were present in all studies, we decided to assess the effects of N. sativa as added to bread (as a regular food) on lipid profiles, apolipoproteins and inflammatory factors in metabolic syndrome patients.
Materials and Methods
Study design
A cross-over, double-blind, and randomized clinical trial was conducted in 54 metabolic syndrome patients of both sexes with age group of 20-65 years old in Chaloos, north of Iran. Our project was approved by medical ethics committee of Isfahan University of Medical Sciences. This clinical trial has been registered in Iranian Registry of Clinical Trials with registration number IRCT2015041821815N1. Subjects were collected according to the data from several laboratories and general recalling. Our criteria for diagnosis of subjects with metabolic syndrome was the definition of NCEP-ATPIII.
Study procedure
After selection of subjects who had essential parameters to be included in the survey, a total of 54 people with metabolic syndrome entered into the study and was referred to School of Medical Science, Azad University of Chaloos as performing center of the study.
All of patients were informed about aims of survey and have accepted a letter of satisfaction from each theme for participating in the study.
Characteristics of subjects include age, gender, level of physical activity, telephone, address, and other information such as current diseases, medication, and history of chronic diseases in family were recorded in a questionnaire.
For evaluating unusual dietary intake, we assessed three dietary food records of the subjects (a weekend and two week days). Patients who had been consumed medicinal plants or their energy intake had been below 1,200 kcal or above 4,000 kcal were excluded from the study.
Each of the patients was served a sample of balanced diet based on food guide pyramid and according to nutritional requirements in order to let them follow a standard diet. Evaluation of daily energy requirement were based on formula suggested by the Institute of Medicine, Food and Nutrition Board [21]. Also, subjects were advised not to change the level of their physical activity during the study.
Preparation of breads
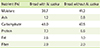
The N. sativa (black seed) was purchased from a local market. After several grinding and screening of seeds, the powder of black seed was delivered to a local bakery which was expert in producing of dietetic breads. It was considered two types of 100 gram massive bread for this study: A bread which include 3 gram of powder of black seed and 3 gram of wheat bran (for intervention group) and the other includes only 3 gram wheat bran and free of black seed (for control group). These breads were prepared by standard bakery materials and methods in hygiene situation and had been under control of the researchers. After cooking, the breads were gradually cooled and put in package. Nutrient composition of two breads was analyzed in food laboratory of School of Nutrition & Food Science, Isfahan University of Medical Sciences and summarized in table 1. According to this table, there is a main difference in fat content of two bread that is due to high polyunsaturated fatty acids in N. sativa.
Randomization and Crossing over
54 patients in this study were divided by regular randomization method in two groups (group A, n = 27 and group B, n = 27).
According to cross-over design in phase 1, one group (for example AB) is assigned as an intervention group and the other (BA) as a control group. After a wash out period, in phase 2 the switch of intervention between groups is done.
Therefore in phase 1, group AB received a 100 grams of bread with N. sativa daily and group BA received the same bread without N. sativa for 2 months. Delivery of breads for patients was performed weekly. After 2 weeks of wash-out period phase 2 started with switching groups as group BA could received breads with N. sativa and group AB received breads without that for 2 month.
Double-blinding
For performing of double-blind status in this study, a third person was recruited who was informed about study groups and type of breads. Delivery of breads to patients was done by this person so the researchers and the subjects were not aware of the type of breads they provide or they received. Although, two types of breads had almost the same shape.
Assessment of variables in study
Before starting phase 1, all of patients were referred to laboratory for measuring of biochemical parameters. Then, in the end of phase 1, beginning and end of phase 2, these assessments were continued.
Measuring of biochemical indices
For measuring of lipid profiles (TG, CHOL, LDL-CHOL, HDL-CHOL), apolipoproteins (APO-A, APO-B), and inflammatory factor (hs-CRP), the subjects were requested to go to laboratory after 10-12 hour of fasting. Samples of subjects were collected from venous blood. Blood samples were centrifuged for 5-7 min at 3,000-g and at 37℃ after 20-30 min of collection time. Serum levels of TG and CHOL were measured in photometric manner and by using commercial kits and HDL-CHOL was measured by enzymatic kit (Pars Azmoon Co, Tehran, Iran). Although LDL-CHOL was calculated with related equation, for adjusting of measurement, a commercial kit was also used (Pars Azmoon Co, Tehran, Iran).
Measuring of APO-A and APO-B in serum were performed in photometric (immunotorbidometric) manner and by using of commercial kits (Pars Azmoon Co, Tehran, Iran).
Serum level of hs-CRP was assessed in immunofloresence manner by using of commercial kit and device of I-Chrome (I-Chrome Co –Seoul-South Korea).
Statisctical analysis
The statistical analysis was performed using SPSS software (version 22). In this crossover study, the comparison of effect of two types of breads (treatment effect), and grouping of subjects (sequence effect) before and after the intervention (time effect) on related parameters were assessed. The general linear model was used for evaluating this effects. A p value of < 0.05 was considered as significant.
Results
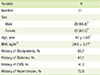
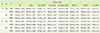
Among the 54 patients with MetS who were included in this study, three subjects were excluded (2 men and 1 woman) due to the change of medication and therapy process (< 6% drop out). Therefore, a total of 51 patients completed the study. Biographic and clinical characteristics of patients are summarized in Table 2. Number of men and women were 29 and 22, respectively. Mean age of the subjects was 47 ± 5.66 years. Mean body mass index (BMI) was 29.9 ± 3.77 kg/m2. Besides, family history of diseases in patients was represented in Table 2. After dividing the patients into two groups (as cross-over study), effects of treatment (two types bread), sequence (grouping of subjects), and time (before and after intervention) of study were assessed. Mean and standard deviation (SD) of biochemical indices were mentioned based on types of treatment (A or B), grouping of patients (AB or BA), and time of measuring of parameters (PRE or POST of intervention) (Table 3).
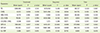
The results showed that treatment, sequence and time have affected blood parameters in MetS patients, but these influences were not mostly significant in many of them. Also, mean of changes in related indices was different based on type of the study effect. The effects of treatment and time were not significant on TG, CHOL, LDL-CHOL, HDL-CHOL, LDL/HDL-CHOL, APO-A, APO-B, and hs-CRP (p > 0.05) but sequence effect was significant on CHOL, LDL-CHOL, APO-A and APO-B (p < 0.05), but was not significant on other parameters (p > 0.05) (Table 4).
Discussion
The aim of this study was to assess effects of bread with N. sativa on lipid profiles, apolipoproteins, and a inflammatory factor in MetS patients in framework of a cross-over study. As it has been mentioned above, these effects in this study were not significant on most of the biochemical parameters. On the other hand, consumption of bread with N. sativa (in comparison of bread without that) does not have a considerable effect on these parameters (treatment effect). Also, there was no significant effect between mean of changes of indices in beginning and end of the study (time effect). But, in regards to grouping of patients to be included in the intervention and control groups first or last, this effect of the study was significant for some of parameters (CHOL, LDL-CHOL, APO-A, and APO-B) and was not in the others (sequence effect). These results were in accordance with the results of some of studies and were opposite to others which assessed the effects of supplementation of N. sativa on lipid profiles. In a study of Najmi et al., N. sativa in spite of change in LDL-CHOL and HDL, could not reduce blood CHOL and TG in MetS patients [22]. Ibrahim et al. [23] also did not find any significant change in blood HDL-CHOL in MetS patients with N. sativa supplementation but found reduction of serum CHOL, LDL-CHOL, and TG. A study of Husseini et al. on type II diabetic patients did not show any significant change in TG, LDL-CHOL, and HDL-CHOL, with consumption of N. sativa and just showed only reduction of CHOL in serum [24]. Dehkordi et al. [25] did not report any change in serum level of TG and HDL-CHOL in patients with mild hypertension by N. sativa supplementation. Also, in a study of Qidwai et al., N. sativa supplementation did not have significant effect on lipid profiles [26]. Therefore, our study results were in accordance with many of others because aspects of change in lipid profiles were not same among the studies.
Several mechanisms are proposed for hypolipidemic effect of N. sativa, for example, enhancing cholesterol metabolism due to rich source of polyunsaturated fatty acids [27], increasing secretion of cholesterol in the bile and hence excretion in feces [28], and reducing serum triglyceride due to presence of Nigellamin that acts like Clofibrate [29].
In spite of mechanisms that is proposed above, in our study (similarity to several studies as mentioned above), bread with N. sativa did not have significant effect neither on lipid profiles nor on apolipoproteins. As it was mentioned before, APO-A and APO-B were respectively connected to serum HDL-CHOL and LDL-CHOL. It is possible that due to no significant change in other lipid indices, changes in serum APO-A and APO-B were not considerable.
Of course, in all of studies that assessed effects of N. sativa on clinical and biochemical indices, form of supplementation was pharmacological but in this study we used food form of N. sativa. Thus, it is possible that food intervention has different effects in comparison to pharmacological intervention.
Several reasons could be propose for no effect of bread with N. sativa on lipid profiles and apolipoproteins :
Positive sequence effect that was acquired in our crossover study on some of parameters (CHOL, LDL-CHOL, APO-A and APO-B), means that patients who started the study firstly as intervention group (in phase 1) and after as control group (phase 2) got significant changes in these indices compared with patients who started inversely. Although, treatment and time effects of our cross-over study did not show overall any significant changes in lipid profiles and lipoproteins by consumption of bread with N. sativa.
Our study did not show a significant change in inflammatory factor (hs-CRP). This result is similar to the report of Datau et al. which showed N. sativa supplementation could not reduce significantly serum hs-CRP in subjects with obesity [20] but was opposite to a study of El-deep which showed N.sativa supplementation reduced serum CRP in patients with coronary artery diseases [19]. It was proposed that N. sativa presented anti-inflammatory effect by inhibition of arachidonic acid metabolism [19], but this was not significant in our study. Perhaps, the reasons which are mentioned above in regards to lipid profiles represented here. Also, clinical status of patients may affect this effect, in the study of El-Deeb [19], patients suffered from an artery disease that includes an inflammatory condition such as atherosclerosis, however our study was performed with patients with MetS that we did not know exactly about their inflammation situation. Therefore it is possible that anti-inflammatory effect shows up in presence of an inflammatory condition [31].
Conclusion
We can conclude from this cross-over study that in spite of significant sequence effects of bread with N. sativa on some of biochemical indices (CHOL, LDL-CHOL, APO-A, and APO-B), treatment and time effects of this study on lipid profile (TG, CHOL, LDL-CHOL, and HDL-CHOL), LDL/HDL-CHOL, apolipoproteins (APO-A and APO-B) and inflammatory factor (hs-CRP) were not significant metabolic syndrome patients .
As this study is one of the most newest trial in the field of food form of N. sativa supplementation, it is proposed that the performance of further studies in this field can reveal clearly the therapeutic effects of this seed.
 XML Download
XML Download