

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Inflammation, oxidative stress and disturbances of zinc homeostasis may play a pivotal role in the pathogenesis and progression of type 2 diabetes mellitus (T2DM) [12]. Low zinc status is associated with a decrease in insulin sensitivity, impaired glucose utilization, inflammation and oxidative damage [3]. Despite the well-established relationship between zinc transporter 8 (ZnT8) and diabetes, a reliable diagnostic tool to access zinc status is still lacking [4]. Metallothionein (MT) and zinc transporters (ZnTs) have been studied recently as possible biomarkers related to body zinc status [5]. Nevertheless, the understanding of the relationships between ZnTs and T2DM is limited, and the impact of diet on genes related to inflammation and oxidative stress in T2DM is still poorly understood. Moreover, nutrition is probably the most important environmental factor, which is able to modulate expression of genes involved in metabolic pathways associated with T2DM [6], and this highlight the importance of a proper diet as a nutrition therapy. Thus, this study was aimed at evaluating the effect of a one-week balanced diet on metabolic control and the expression of ZnTs in peripheral blood mononuclear cells from patients with T2DM.
Materials and Methods
Participants and Study Design
We recruited patients with T2DM from the Nutrition and Endocrinology assistance service at the Federal University of Rio Grande do Norte (UFRN), Natal, Brazil. The recruitment was performed using the medical records. Inclusion criteria were as follows: (1) age of 18-60 years; (2) T2DM diagnosed within 1-5 years; (3) last HbA1C measurement ≥ 6.5%; and (4) no change in hypoglycemic medication for at least 3 months before entering the study. Exclusion criteria were as follows: (1) diabetic complications (neuropathy, retinopathy, renal disease); (2) current insulin treatment; and (3) routine consumption of nutritional supplements. We identified 93 patients with T2DM, 41 of whom met the inclusion criteria and 12 of those agreed to participate. Among them, 2 patients were lost due to noncompliance, leaving 10 patients enrolled. We also recruited 5 healthy volunteers just to provide anthropometric, biochemical and molecular data at baseline as a control group. These eutrophic volunteers were employees of the university where the studied was performed, with ages between 18-60 years, and with normal values for fasting plasma glucose (< 100 mg/dL) and HbA1c (< 6.5%). The study protocol was reviewed and approved by the ethics committee of the UFRN (208.133/13). All subjects provided written, informed consent before enrollment. An individualized dietary intervention was implemented for one week on patients with T2DM. Nutritional assessment and blood collection were performed before (T0) and after (T1) the intervention. Prior to the dietary intervention, food intake was obtained using food records (Figure 1).
Food Intake
Information on food intake was obtained using food records from 3 nonconsecutive days (2 weekdays and 1 weekend day). Patients received three 24-hour food record forms to record, all of the foods and beverages consumed, as accurately as possible. As recommended by Thompson and Byers [7], trained dietitians instructed the patients on how to properly record their food intake, including information about time, description of food and eaten amount. The household measures of foods were converted to grams or volume scale prior to being analyzed. Energy, protein, fat, carbohydrates, total fiber, calcium, iron, and zinc intakes were calculated using AVANUTRI Revolution® Software (Avanutri, Rio de Janeiro, Brazil). Foods not included in the software were incorporated to analysis based on Brazilian food composition table [8] or on nutritional information contained on the food labels.
Dietary Intervention
The individualized eating plan was based on recommendations by the American Diabetes Association [11] and the Brazilian Diabetes Society [12]. A normocaloric diet (25-30 kcal/kg/day) for weight maintenance, containing 20% of energy as protein, 20% as fat, with low levels of saturated fatty acids (SFA), and 60% as carbohydrates with high fiber was provided for T1. The diet included carbohydrate from fruits, vegetables, whole grains, legumes, fiber-containing foods, and low-fat milk. Trans fat was minimized. Sugar was replaced by non-nutritive sweetener. Red meat was offered just two times per week and three servings of fish per week were provided. Extra virgin olive oil was included daily as salads dressing. We offered a diet pattern which is totally accessible and realistic. The diet was provided and not only prescribed, with eliminating possible bias. Food and meals were delivered to patients' homes every other day.
Sample Collection and Processing
After an overnight fasting, blood samples were collected in specific tubes (Vacutainer, BD Diagnostics, Sparks, MD, USA), to perform hematological analysis and to obtain sera and peripheral blood mononuclear cells (PBMCs), as previously described [5]. Fasting plasma glucose (FPG) and glycated hemoglobin (HbA1c) were measured by automated enzymatic methods (ABX Micros 60, Horiba Medical Diagnostics, Montpellier France), plasma tumor necrosis factor α (TNFα) and plasma interleukin 6 (IL6) were measured by chemiluminescence (IMMULITE® 1,000 Immunoassay System, Siemens Healthcare, Malvern, PA, USA). Serum zinc (SZn) was measured by atomic absorption spectrophotometry (Varian SpectrAA 220 FS, Australia) and gene expression by qPCR (StepOnePlus real time PCR system, Applied Biosystems, Foster City, CA, USA), according to the manufacturer's instructions. Purification of RNA from PBMC was performed using the AllPrep DNA/RNA/Protein Mini Kit (Qiagen, USA). Reverse transcription reaction was performed using a set of High Capacity cDNA Archive Kit (KITS) (Applied Biosystems, Foster City, CA, USA). For analyses of ZnTs, TNFα, IL6 and Metallothionein 1 (MT1) mRNAs primers and probes were used together with TaqMan reagents (Life Technologies, Road Grand Island, NY, USA). Primers and TaqMan probes were designed by using PRIMER EXPRESS, version 3.0 (Applied Biosystems, Foster City, CA, USA). The levels of mRNA expression were normalized to 18S rRNA expression as an endogenous reference and quantified using the crossing point difference method.
Statistical Analysis
Results are shown as mean ± SD. The Shapiro-Wilk test was used to analyze the normality of the data. To compare means between T0 and T1 (paired data) (Table 1 and Figure 2), we used the Student t test or Wilcoxon test, according to the data distribution. The Pearson or Spearmen correlation test was used to analyze the association between each pair of gene expression studied (Table 2), depending on whether or not the data was normally distributed. Furthermore, to compare differences between two independent groups (ex. healthy subjects vs. T0) (Figure 2) not normally distributed, we used Man-Whitney test. Statistical analysis was performed using Graph Pad-Prism v.6.0a and changes were considered significant if p ≤ 0.05.
Results and Discussion
Anthropometric and Biochemical Data
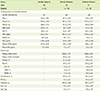
Greater body weight, BMI, %FM, FPG, and plasma TNFα and IL6 were found in diabetic patients (T0) compared to healthy subjects (Table 1). Obesity and pro-inflammatory cytokines including TNFα and IL6 can enhance insulin resistance and impair glucose homeostasis [13]. The greater levels of plasma TNFα and IL6 found in diabetic patients reveal a typical inflammatory profile of these patient. Consistent with our results, higher levels of TNFα have been found in postmenopausal woman [14] and in both male and female diabetic patients [15].
After the balanced diet was provided to the diabetic patients (T1), plasma TNFα and IL6 levels tended to decrease, but the difference was not significant (Table 1). The one-week intervention might have been too short to detect significant changes in these parameters. On the contrary, the FPG of diabetic patients decreased significantly at T1. However, no weight change was observed in our diabetic patients (Table 1), emphasizing the importance of the diet composition and not only a caloric restriction on glycemic control of diabetic patients [16].
Participants of all groups had SZn concentration above the suggested lower cutoff value for low zinc status (Table 1). Studies have shown both decreased [117] and increased [1819] levels of SZn in diabetic patients. In general, a decrease of SZn is common in T2DM due to hyperzincuria, whereas an increase of SZn is seen more often in type 1 diabetes due to a destruction of pancreatic β-cells with release of zinc [20]. Furthermore, SZn concentrations might be dependent on the age of diabetes occurs [2] and on the duration of diabetes: the level of SZn decreases with longer duration of diabetes [20]. SZn is not a reliable biomarker to evaluate body zinc status [21]. Since the diabetic patients have normal SZn in this study, the elevated inflammatory mediators may not have been at levels needed to induce hypozincemia [2223]. Comparing the balanced diet (T1) with the usual diet (T0) in diabetic patients, there were significant differences in total fat and SFA, and a significant increase of carbohydrate, fiber, calcium and iron intake (Table 1).
Expression of Zinc Transporters in PBMC
Patients with T2DM showed lower expression of ZnT4 mRNA and higher IL6 mRNA compared with healthy subjects (Figure 2). Comparing T0 and T1, we observed down-regulation of TNFα, IL6 and MT1 mRNAs in response to the balanced diet intervention (Figure 2). Nevertheless, ZnT4 mRNA was not different between T0 and T1 in this study. Of note, Noh et al. [24] found a down-regulation of ZnT4 mRNA expression in obese women with high levels of plasma TNFα. As a zinc exporter protein, a decrease of ZnT4 mRNA expression in diabetics compared to healthy individuals might influence inflammation by increasing retention of intracellular zinc.
A zinc depletion and repletion study demonstrated a modulated expression of ZnTs and inflammatory genes in blood cells from nine healthy men [5]. Conversely, a 12-week trial did not show any significant difference in expression of ZnTs and MT after zinc and/or α-linolenic acid supplementation [14]. In our study, ZnTs expression did not change in response to an intervention of one-week balanced diet (Figure 2). However, down-regulation of TNFα, IL6 and MT1 were observed at T1 in response to diet without a change in medical therapy or physical activity level. Our findings are in agreement with studies, which have reported that healthy food choices improve glucose metabolism and dampen inflammation, thereby repress the expression of pro-inflammatory genes [2526]. In addition, considering that a MT is a redox-active protein, and is induced during inflammation, the down-regulation of MT1 mRNA found at T1 indicates a reduction of oxidative stress [27].
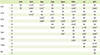
A range of bivariate correlations in transcripts from PBMC was found in Table 2. Previous studies found positive associations among ZnTs mRNAs in healthy young adults (ZnT1 vs. ZnT5, and ZnT1 vs. Zip3) [26], and in diabetic women with T2DM after (Zip3 vs. Zip5) or without zinc supplementation (ZnT6 vs. Zip7) [14]. In agreement with Foster et al. [28], we observed the greatest association among ZnT1, Zip3 and ZnT5 mRNA. Expression of this cluster of ZnTs behaved in a similar manner in patients with T2DM. Furthermore, TNFα mRNA was highly associated with ZnT1 and MT1 transcripts, whereas IL6 mRNA had a strong correlation with Zip8 and Zip14. This finding is in agreement with the documented regulation of these transponder genes by proinflammatory cytokines [21]. Noteworthy, all positive associations involving MT1 mRNA was found only at T1, implicating that MT1 expression is sensitive to glycemic levels (Figure 2).
Conclusions
A balanced diet provided for one week was able to improve metabolic control in patients with T2DM by lowering FPG. This metabolic control may be related to down-regulation of zinc-related transcripts from PBMCs, as changes of TNFα, IL6 and MT1 mRNA. The dietary intervention was not able to provide a significant change on ZnTs mRNA from PBMC in this study.
The limitations of the present study include its small sample size and a short study period. Additional studies are required to better understand the impact of diet on ZnTs and its effects on metabolic and inflammatory pathways in adults with T2DM.


 XML Download
XML Download