

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of diabetes has been rising in modern society and, the number of people with type 2 diabetes is rapidly increasing in the recent decades [1]. In Korea, the mortality rate from diabetes has also increased rapidly from 7.4% in 1988 to 25% in 2003 and has kept about 20% since 2004 [2]. Furthermore, the consequent micro- and macro-vascular complications may influence a significant economic impact as well as cause the increase of morbidity and mortality [1]. Diabetes is known to be associated with multiple risk factors of coronary heart diseases including hypertension, dyslipidemia and abnormalities in hemostasis and cardiac function [34].
It is clear that a strong link exists between perturbations in insulin signal transduction and alterations in lipid and lipoprotein metabolism [5]. A central initiating factor appears to be defects in the storage and oxidation of free fatty acids (FFAs) [5]. These initial abnormalities appear to lead to hepatic and intestinal overproduction of highly atherogenic lipoprotein particles that result in the commonly observed phenotype of hypertirglyceridemia, hyperapolipoprotein B, low levels of high density lipoprotein-cholesterol (HDL-C) [5]. Even though low density lipoprotein cholesterol (LDL-C) is known as an established risk factor for atherosclerosis [6], many of recent studies reported that apolipoprotein B (ApoB) is a better measure of cardiovascular disease (CVD) risk than LDL-C [678910], because ApoB indicates the number of potentially atherogenic lipoprotein particles [11]. Emerging evidences have demonstrated that ApoB may be a significant predictor of CVD risk in subjects carrying metabolic syndrome (MetS), which is consistent with the reports from multiple studies performed in populations with MetS or its features, which also demonstrate the ApoB-associated risk [10]. Furthermore, the measure of ApoB may be relevant in the setting of insulin resistant (IR) states, because patients with diabetes or MetS often manifest normal LDL-C values, but have a preponderance of small, dense LDL particle and higher ApoB levels [6]. Recently, Salomaa et al. [12] reported in his large cohort studies (Finnish), that ApoB and adiponectin among the screened 31 novel biomarkers were best biomarkers for the prediction of the risk of incident diabetes in both men and women. Adiponectin is an insulin sensitizing adipocytokine which exerts anti-atherogenic and anti-inflammatory effects [1314]. Plasma adiponectin levels are decreased in obesity [15], type 2 diabetes [16], and hypertension [17]. In addition, apolipoprotein A1 (ApoA1) which reflects antiatherogenic high density lipoprotein (HDL) particles is also thought to accurately indicate the cardiovascular risk than LDL-C or other lipids [9]. According to Matsumoto et al., serum ApoB levels and ApoB to ApoA1 (ApoB/ApoA1) were better predictors of atherosclerotic vascular disease, compared with LDL-C [10]. Also, the combination of ApoB and IR estimated by homeostasis model assessment (HOMA) is thought to be a superior marker of atherosclerosis than LDL-C alone in patients with type 2 diabetes [8]. However, most studies were performed in diabetic patients. Furthermore, there is no study on the association between Apo B and the risks of diabetes in non-diabetic Koreans [18]. Therefore, this study aimed to investigate the association of serum ApoB concentrations with the risk of diabetes in Korean men through the cross-sectional and short-term observational studies.
MATERIALS AND METHODS
Study population
All study participants were recruited from the Health Service Center (HSC) in the course of a routine checkup visit or by a newspaper announcement for health examination. None of study subjects had history of diagnosis of impaired glucose tolerance (IGT) or diabetes before participating in the study. In addition, subjects were excluded if they have orthopedic limitations, weight loss/gain (10%) over the previous 6 months, or any diagnosis of vascular disease, cancer (clinically or by anamnesis), renal disease, liver disease, thyroid disease, and acute or chronic inflammatory diseases. In addition, MetS was assessed by the Korean guideline. The definition includes at least three components (1) waist circumference ≥ 90 cm for men and ≥ 85 cm for women, (2) triglyceride (TG) ≥ 150 mg/dL, (3) HDL-cholesterol < 40 mg/dL for men and < 50 mg/dL for women, (4) blood pressure (BP) ≥ 130 / ≥ 85 mmHg and (5) fasting glucose ≥ 100 mg/dL. Subjects with fasting glucose between 100 and 126 mg/dL were classified to IFG and those with fasting glucose ≥ 126 mg/dL were classified to DM. After the screening test, those with fasting glucose between 100 and 125 mg/dL were classified into impaired fasting glucose (IFG) and those with fasting glucose ≥ 126 mg/dL were classified into newly-onset diabetes. None of study subjects were taking medications (i.e. antihypertensive, antidyslipidemic, antithrombotic and antidiabetic drugs). When the fasting glucose levels are werearound the borderline (i.e. 98, 99, 100, 101 or 102 for IFG; 124, 125, 126, 127 or 128 for diabetes), glucose levels were retested twice more in another days to make it confirmed for confirmation. Finally, 790 genetically unrelated Korean men were included in the analysis (40-79 years); According to their fasting blood glucose levels, 519 subjects were categorized into normal fasting glucose (NFG), 188 were IFG and 83 were newly-onset diabetes. In addition, NFG subjects did not have MetS. Among the subjects with NFG or IFG at the beginning of the study, those who had agreed to the second examination were re-investigated after 3 months in order to investigate the relationship between the changed ApoB levels and the increased risk of hyperglycemia. Written informed consent was obtained from all subjects and the protocol was approved by the Institutional Review Board of Yonsei University.
Anthropometric parameters and blood pressure measurements
Body weight and height were measured in the morning, light clothed without shoes. Body weight was measured using a TBF-105 body fat analyzer (Tanita Corp., Tokyo, Japan) and standing height was measured using a wall stadiometer. The body mass index (BMI) was calculated as body weight in kilograms divided by height in square meters (kg/m2). Blood pressure (BP) was obtained from the left arm of seated patients with an automatic blood pressure monitor (TM-2654, A & D, Tokyo, Japan) after 20 minutes of rest. The average of three measurements was recorded for each subject.
Blood collection
After a 12-hour fasting period, venous blood specimens were collected in EDTA-treated and plain tubes. The tubes were immediately placed on ice in the dark until they arrived at the analytical laboratory (within 1–3 hours). Then, the blood specimens were centrifuged into plasma or serum then, stored at -70°C until analysis.
Lipid profile and apolipoproteins
Fasting serum total cholesterol, TG and FFA were measured using commercially available kits on a Hitachi 7150 Autoanalyzer (Hitachi Ltd., Tokyo, Japan). After precipitation of serum chylomicron, LDL and very low density lipoprotein (VLDL) with dextran sulfate-magnesium, HDL-C left in the supernatant was measured by an enzymatic method. LDL-C was estimated indirectly using the Friedewald formula for subjects with serum TG concentrations < 400 mg/dL (4.52 mol/L). In subjects with serum TG concentrations ≥ 400 mg/dL (4.52 mol/L), LDL-C was measured by an enzymatic method on a Hitachi 7150 Autoanalyzer directly. Each sample was measured duplicate and their average value was used for one value. Serum apolipoprotein A1 and B were determined by turbidometry at 340 nm using a specific anti serum (Roche, Basel, Switzerland).
Glucose, insulin and HOMA-IR
Fasting glucose was measured by a glucose oxidase method using the Beckman Glucose Analyzer (Beckman Instruments, Irvine, CA, USA). Insulin was measured by radioimmuno-assays with commercial kits from Immuno Nucleo Corporation (Stillwater, MN, USA). Insulin Resistance (IR) was calculated with the HOMA (Homeostasis Model of Assessment) using the following equation:
Plasma adiponectin concentration
Plasma adiponectin concentration was measured using an enzyme immunoassay (Human Adiponectin ELISA kit, B-Bridge International Inc., Cupertino, CA, USA). All these assays were read using a Victor2 (Perkin Elmer life sciences, Turku, Finland) at 450 nm and wavelength correction was set to 540 nm.
The assessment of dietary intake and energy expenditure
Information on each subject's usual diet was obtained from a 24-hour recall method. All the subjects were given written and verbal instructions by a registered dietitian on completion of a recent 3-day (2 week days and 1 weekend) dietary intake. Dietary energy values and nutrient content were calculated using the Computer Aided Nutritional Analysis Program (CAN-pro 2.0, Korean Nutrition Society, Seoul, Korea). Total energy expenditure (TEE) (kcal/day) was calculated from activity patterns including basal metabolic rate, physical activity for 24 hours [19], and specific dynamic action of food. Basal metabolic rate for each subject was calculated with the Harris-Benedict equation [20].
Statistical analysis
Statistical analyses were performed with SPSS version 15.0 for Windows (Statistical Package for the Social Science, SPSS Ins., Chicago, IL, USA). One-way analysis of variance (ANOVA) followed by Bonferroni method was used to compare the difference in the continuous variables among the subject groups. Frequencies were tested by χ2 test among groups. Pearson correlation analysis was performed to examine the relationship among the variables. The association of ApoB levels with the increased risk of IFG or newly-onset diabetes was calculated using the odds ratio (OR) [95% Confidence intervals (CIs)] by a multiple logistic regression analysis with adjustment for confounding factors (i.e. age BMI, systolic BP, diastolic BP, TG, HDL-C, LDL-C, non-HDL-C, ApoA1, adiponectin etc. which were positively correlated with ApoB and fasting glucose, Supplementary Table 1). Hosmer-Lemeshow test for goodness of fit for logistic regression was performed (p value = 0.753, c2 value: 4.991). Multiple stepwise regression analysis was performed to find a main contributor to the increased risk of hyperglycemia after 3 months' follow-up. Before statistical testing, each variable was examined if it presented normal distributions; the skewed variables were logarithmically transformed and then tested. For descriptive purposes, mean values are presented using untransformed and unadjusted values. Results are expressed as mean ± S.E or %. A two-tailed value of p < 0.05 was considered statistically significant.
RESULTS
Clinical and biochemical characteristics of the study groups
Table 1 shows clinical characteristics of 790 study subjects; NFG (n = 519), IFG (n = 188) and newly-onset diabetes (n = 83). No significant differences were found in age and proportions of cigarette smoking and alcohol consumption among the three subject groups. Mean values of BMI, waist circumference and BPs were significantly lower in NFG subjects compared to those with IFG or newly-onset diabetes. Regarding lipid profiles, the levels of TG, non-HDL-C and ApoB were significantly lowest and the levels of HDL-C were significantly highest in NFG subjects. The levels of glucose, insulin, FFA and HOMA-IR were significantly lowest in NFG subjects, and significantly highest in subjects with newly-onset diabetes. In addition, plasma adiponectin levels were lowest in newly-onset diabetic subjects among the subject groups. No significant differences were observed for dietary intake and energy expenditure among three subject groups.
Table 1
Demographic and metabolic parameters of study population

Mean ± S.E.
Apo, apolipoprotein; BMI, body mass index; DBP, diastolic blood pressure; FFA, free fatty acid; HDL-C, high density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment of insulin resistance {fasting insulin (μIU/mL) × fasting glucose (mmol/L)}/22.5; IFG, impaired fasting glucose; MetS, metabolic syndrome; LDL-C, low density lipoprotein cholesterol; NFG, normal fasting glucose; SBP, systolic blood pressure; TEE, total energy expenditure; TEI, total energy intake; TG, triglyceride.
*Tested by log-transformed, tested by one-way analysis of variance (ANOVA) followed by Bonferroni method.
![]()
Association of ApoB levels with the increased risk of diabetes
In order to examine the association of ApoB levels with the increased risk of diabetes, we divided study subjects into two groups according to ApoB levels (median value) [high-ApoB ≥ 87.0 mg/dL (n = 399) vs. low-ApoB < 87.0 mg/dL (n = 391)] and then, calculated odds ratios (ORs) for the risk of newly-onset diabetes (Table 2). NFG subjects with low-ApoB were considered as a reference group. Subjects with high-ApoB showed a significantly higher risk of newly-onset diabetes [OR0: 2.392, (95% CI: 1.470-3.893), p < 0.001] than those with low-ApoB. This association was still maintained after the adjustment for age and BMI [OR1: 2.228, (95% CI: 1.362-3.646), P1 = 0.001] and further adjustment for systolic BP, diastolic BP, TG, HDL-C, LDL-C, non-HDL-C and adiponectin [OR2: 1.984, (95% CI: 1.001-4.064), P2 = 0.049]. For the risk of IFG, subjects with high-ApoB showed a higher risk than those with low-ApoB before and after the adjustment [OR0: 1.718 (95% CI: 1.225-2.408), P0 = 0.002, OR1: 1.535 (95% CI: 1.087-2.167), P1 = 0.015, respectively], but the significance for the association disappeared after further adjustment for [OR2: 0.912 (95% CI: 0.912-1.609), P2 = 0.9591].
Table 2
Odds Ratios (ORs) for IFG and newly-onset diabetes according to ApoB levels
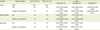
IFG, impaired fasting glucose; DM, diabetes mellitus; MetS, metabolic syndrome; CI, confidence interval; OR0, unadjusted; OR1, adjusted for age and body mass index; OR2, adjusted for age, body mass index, blood pressure (systolic and diastolic), triglyceride, HDL-cholesterol, LDL-cholesterol, non-HDL cholesterol, apolipoprotein A1, and adiponectin.
*Reference group (lower median value)
![]()
In addition, the association between higher ApoB and the risk of diabetes was much greater in subjects with MetS [OR1: 2.805 (95% CI: 1.137-5.737), P1 = 0.005] than in those without [OR1: 1.917 (95% CI: 0.989-3.718), P1 = 0.054].
Relationship between changed levels of ApoB and the increased risk of hyperglycemia
In order to investigate the relationship between the changed levels of ApoB and the increased risk of hyperglycemia during the short period, we further investigated subjects with NFG (n = 77) or IFG (n = 27) who agree to the reinvestigation after 3 months from the participation in the study. By the time of reinvestigation Thirteen of NFG subjects had turned into IFG (16.9%) and 7 of IFG subjects turned into diabetes (25.9%). Among NFG subjects at the initial, fasting ApoB and glucose levels were increased in those who were developed to IFG compared with those who maintained NFG after 3 months (ApoB: 7.23 ± 3.77 vs. -0.08 ± 1.72 mg/dL; glucose: 18.23 ± 2.05 vs. 1.08 ± 0.91 mg/dL, respectively). Among IFG subjects at the initial, fasting ApoB and glucose levels were increased in those who were developed to diabetes compared with those who maintained IFG or got back to NFG after 3 months (ApoB: 1.17 ± 6.36 vs. -4.75 ± 2.58 mg/dL; glucose: 10.3 ± 6.90 vs. -3.75 ± 1.72 mg/dL, respectively).
Multiple stepwise regression analysis was performed in order to find main contributors to the net change of glucose levels (Table 3). Changed glucose levels were a dependent variable, and age, changed levels of BMI, waist circumference, systolic BP, diastolic BP, TG, total cholesterol, HDL-C, LDL-C, non-HDL-C, ApoB, ApoA1 and adiponectin were independent variables. As shown in Table 3, changed levels of ApoB and waist circumference were revealed as major contributors to the net change of glucose levels. In model 1, increased ApoB levels contributed to the increase of fasting glucose levels (standardized b-coefficient: 0.315, p = 0.002;). In model 2, increased levels of ApoB (standardized b-coefficient: 0.281, p = 0.005) and waist circumference (standardized b-coefficient: 0.219, p = 0.029) contributed to the increase of fasting glucose levels, respectively (r = 0.382, p = 0.001).
Table 3
Multiple stepwise regression analysis to find major contributors to the increase of fasting blood glucose level during the short period (3 months)

| Variables | Standardized β-coefficients | p value | R | p value | |
|---|---|---|---|---|---|
| Model 1 | |||||
| ΔApoB | 0.315 | 0.002 | 0.315 | 0.002 | |
| Model 2 | |||||
| ΔApoB | 0.281 | 0.005 | 0.382 | 0.001 | |
| ΔWaist circumference | 0.219 | 0.029 | |||
Dependent variable: changed levels of fasting blood glucose; Independent variables: changed levels of body mass index, waist circumference, systolic blood pressure, diastolic blood pressure, triglyceride, total cholesterol, HDL-cholesterol, LDL-cholesterol, non-HDL-cholesterol, ApoB, ApoA1 and adiponectin; Δ, changed levels between at baseline and after 3-month.
![]()
DISCUSSION
This study suggested that serum ApoB levels may be closely associated with the increased risk of diabetes in Korean men. In our study, subjects with higher ApoB levels (≥ 87.0 mg/dL) showed approximately 2 times higher risk of newly-onset diabetes than those with lower ApoB levels (< 87.0 mg/dL) even after the adjustment for age, BMI, BPs, TG, HDL-C, LDL-C, non-HDL-C, ApoA1 and adiponectin. In addition, multiple stepwise regression analysis revealed that changed ApoB levels were a main contributor to the changed glucose level.
Recent studies have reported that ApoB levels were associated with diabetes [8122122]; for example, plasma ApoB levels was associated with the incidence of type 2 diabetes, and the risk of diabetes might be better predicted by ApoB levels than by LDL-C or HDL-C. These reports may suggest the potential for the use of ApoB in the assessment for the risk of type 2 diabetes [2122]. In a large Finnish cohort studies, Salomaa et al. [12] found that ApoB and adiponectin among the screened 31 novel biomarkers, were the best biomarkers for the prediction of the risk of diabetes incidence. On the other hand, Davidson [5] demonstrated that the predictive value of the ApoB/ApoA1 might be stronger and better than the use of either apolipoprotien alone or together. According to Harper and Jacobson [11], the levels of non-HDL- C strongly correlated with the levels of ApoB, and both of non-HDL- C and ApoB rather than LDL-C, may better predict overall cardiovascular risk. Non-HDL-C is calculated by subtracting HDL-cholesterol from total cholesterol, and it reflects circulating levels of the atherogenic ApoB-containing lipoproteins including LDL-C, VLDL, intermediate density lipoprotein cholesterol, chylomicron remnants, and lipoprotein(a) [1123]. Non-HDL-C has as a major advantage in aspect that it can be calculated by all lipid profiles, and it measures all the ApoB-containing lipoproteins that are considered atherogenic [23].
In our study, serum ApoB levels turned out to be a good predictor for the risk of newly-onset diabetes even after the adjustment. In addition, net change of ApoB levels together with that of waist circumference were found as main influencing factors on the net change of glucose levels. It may be related that an absolute value of ApoB indicates the particle number of LDL as well as represents approximate LDL size thus, the measurement of ApoB levels may better reflect diabetic status, particularly newly-onset diabetes [613].
The present investigation may have several limitations. First, the study design was rather based on cross-sectional observation, not on a case-control design, because study participants (NFG, IFG and newly-onset diabetes) were classified by screening their fasting glucose levels even though some people were in the borderline of criteria had re-examination. Second, the period of follow-up observation (3 months) was so short, and the followed-up sample size was small. Thirds, study subjects were exclusively Korean men, thus the results may not be applicable to women or other ethnic samples whose clinical and biochemical characteristics may differ from those in our population. Thus, it is necessary to investigate the relationship between ApoB levels and the risk of newly-onset diabetes in other ethnic population as well as much larger population including women. In addition, prospective longitudinal observation is needed in order to investigate if ApoB levels can be used as a better prognostic marker for the risk of newly-onset diabetes and diabetic complication.
 XML Download
XML Download