

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Blood or dietary fatty acids (FAs) were associated with metabolic disorder such as metabolic syndrome (MS), diabetes and cardiovascular disease (CVD) [1234]. The features of MS (i.e. insulin resistance, IR, dyslipidemia, smaller LDL particle size, decreased adiponectin and increased inflammation and oxidative stress) linked to cardiovascular risk were significantly related with serum phospholipid FA compositions and the severity of arterial stiffness [345]. Dietary n-3 long-chain polyunsaturated FAs (LC-PUFAs; i.e. eicosapentaenoic acid, EPA and docosahexaenoic acid, DHA) are associated with IR [6], blood pressure (BP) [7] and vascular aging [8]. Tomiyama et al. [8] reported that daily consumption of 1.8 g EPA for 12 months ameliorated arterial stiffness in patients with dyslipidemia. In our previous study, coronary artery disease (CAD) patients with MS show low proportion of PUFAs, particularly DHA in serum phospholipids [9] than the counterparts. Additional in vitro experiment shows that DHA treatment plays a protective role in LPS-induced vascular smooth muscle cell (VSMC) proliferation and inflammatory response by regulating ERK, p38 and NF-κB/p65 signaling pathways [9].
Numerous longitudinal and prospective studies reported the association of n-3 FAs intake with reduced CVD mortality [10]. A meta-analysis of randomized controlled trials also demonstrated that taking ≥ 3 g of n-3 LC-PUFAs/day by fish-oil supplements lowered BPs particularly in the middle aged and elderly people [11]. On the other hand, dietary intake of n-3 PUFAs ≤ 1 g/day for 12 months in healthy adults did not improve endothelial function expressed by brachial artery flow-mediated dilation (ba-FMD), arterial stiffness and BPs [12]. It was consistent with cross-sectional survey in 3,045 adults (45-84 years) [13] showing no significant relation between n-3 PUFAs intake with ba-FMD. Two more studies did not show any effects of n-3 PUFA injection (1.3-3.0 g/day for 3-12 weeks) on endothelial activation markers in young (≤ 45 years) [14] and middle-aged (50-70 years) [15] people.
However, the results are still controversial, and only a few studies have investigated the association of LC-PUFAs with cardiovascular risk parameters including vascular functions in healthy people. Therefore, this study aimed to investigate if serum phospholipid LC-PUFAs, particularly DHA are associated with the alteration of cardiovascular risk parameters and vascular function in metabolically healthy people. We hypothesized that lower proportions of LC-PUFAs particularly DHA in serum phospholipids are significantly associated with the increased risk of CVD and affect vascular function in metabolically healthy men. To elucidate it, we first compared basic and biochemical parameters related with cardiovascular risk and serum phospholipid FA compositions between healthy men and CAD men without MS, and then performed further analysis on the association of serum phospholipid DHA composition with cardiovascular risk and arterial stiffness in metabolically healthy men.
Go to : 
MATERIALS AND METHODS
Study population
Metabolically healthy men were recruited from the Health Service Center in the course of a routine checkup visit or by a newspaper announcement for health examinations and enrolled to the study (March 2013-March 2014). Those who were electrocardiographically normal were included. Exclusion criteria were orthopedic limitations, weight loss/gain over the previous 6 months, or any diagnosis of vascular disease, diabetes, cancer (clinically or by anamnesis), renal disease, liver disease, thyroid disease, and acute or chronic inflammatory diseases. Subjects with MS were also excluded. MS was defined using a combination and modification of the NCEP-ATPIII guideline, Asian-Pacific guideline and American Diabetes Association guideline [161718]. This definition requires at least three of the following components: waist circumference ≥ 90 cm (men); triglyceride ≥ 150 mg/dL; high density lipoprotein cholesterol (HDL-cholesterol) < 40 mg/dL (men); blood pressure ≥ 130 / ≥ 85 mm Hg; and fasting glucose ≥ 100 mg/dL (but fasting glucoses ≥ 126 mg/mL were considered diagnostic of diabetes). None of participants were taking any medications (antihypertensive, antidyslipidemic, antithrombotic, and antidiabetic drugs).
CAD patients were recruited from the Severance Cardiovascular Hospital, Seoul, Korea. The inclusion criteria were as follows: (1) angiographically confirmed CAD with ≥ 50% occlusion of one or more major coronary arteries, (2) myocardial infarction confirmed according to World Health Organization criteria for symptoms, enzyme elevation, or electrocardiographic changes, (3) absence of non-atherogenic occlusion, i.e. osteal stenosis and spasm, (4) neither orthopedic limitations nor any diagnosis of the diseases mentioned above (diabetes, cancer, and renal, liver, thyroid and acute or chronic inflammatory diseases). CAD patients with MS were also excluded.
Finally, 499 genetically unrelated healthy men and CAD male patients (n = 111) were included in this study (30–69 years). Participation rates in case and healthy subjects from the recruitment were 50% and 70%, respectively. Written informed consent was obtained from all participants, and the study protocol was approved by the Institutional Review Board of Yonsei University.
Anthropometric parameters and blood collection
Height, body weight and waist circumference were measured. Body mass index (BMI) was calculated as body weight/height (kg/m2). Blood pressure (BP) was obtained from the seated individuals with an automatic BP monitor (TM-2654, A&D, Tokyo, Japan) after 20 minutes of rest. Study participants were interviewed regarding their smoking and drinking behavior. After an overnight fast, venous blood specimens were collected in EDTA-treated and plain tubes. The tubes were immediately placed on ice until they arrived at the analytical laboratory (1-3 hours). Then, the blood specimens were separated into plasma or serum, and stored at -80°C until analysis.
Serum lipid profile and free fatty acids
Serum total cholesterol, triglyceride and free FAs (FFAs) were measured using commercially available kits on a Hitachi 7150 Autoanalyzer (Hitachi Ltd., Tokyo, Japan). After precipitation of serum chylomicron, LDL, and VLDL with dextran sulfatemagnesium, HDL-cholesterol left in the supernatant was measured by an enzymatic method. LDL-cholesterol was calculated indirectly using the Friedewald formula for individuals with serum triglyceride < 400 mg/dL (4.52 mol/L).
Glucose, insulin, and HOMA-IR
Fasting glucose was measured by a glucose oxidase method (Glucose Analyzer Beckman Instruments, Irvine, CA, USA). Insulin was measured by radioimmuno-assays with commercial kits (Immuno Nucleo Corporation, Stillwater, MN, USA). IR was calculated with the homeostasis model assessment using the following equation: IR = [fasting insulin (mIU/mL) - fasting glucose (mmol/L)] / 22.5.
Liver and kidney functional markers
Serum aspartate aminotransferase (AST) and alanine aminotransferase (ALT) were measured using a modified International Federation of Clinical Chemistry (IFCC) UV method. Serum creatinine was measured with a kinetic colorimetric (Jaffe) assay. Serum blood urea nitrogen (BUN) and uric acid were measured using a kinetic UV Assay.
Plasma adiponectin and LDL particle size, and serum high sensitivity C-reactive protein
Plasma adiponectin concentrations were measured using an enzyme immunoassay (Human Adiponectin ELISA kit, B-Bridge International Inc., San Francisco, CA, USA; Mercodia, Uppsala, Sweden, respectively) and read by a Victor2 (Perkin Elmer Life Sciences, Turku, Finland). Particle size distribution of LDL (density 1.019-1.063 g/mL) isolated by sequential flotation ultracentrifugation was examined using a pore-gradient lipoprotein system (CBS Scientific, San Diego, CA, USA). Serum hs-CRP was measured with an ADVIA 1650 (Bayer, Tarrytown, NY, USA) using a commercially available, high-sensitivity CRP-Latex (II) X2kit (Seiken Laboratories Ltd., Tokyo, Japan). The intra-assay and inter-assay coefficients of variance were 1.87% and 1.89%, respectively.
Fatty acid composition in serum phospholipids
Total lipids in serum were extracted with chloroform/methanol (2:1, v/v) as described by Folch et al. [19]. The phospholipid fraction was isolated from total lipids using thin-layer chromatography and then methylated during 1 hour at 95°C. FA methyl esters were measured with gas chromatography (Hewlett Packard 5890A, Palo Alto, CA, USA) using wax column (Omegawax 320, 30 m × 0.32 mm × 0.25 μm, Supelco, Bellefonte, PA, USA). Individual FAs were calculated as a relative percentage of the total of 26 FAs (set as 100%) using Chemstation software (Hewlett Packard).
Brachial-ankle pulse wave velocity
Brachial-ankle pulse wave velocity (ba-PWV) as a marker for arterial stiffness was measured using an automatic waveform analyzer (model VP-1000; Nippon Colin Ltd., Komaki, Japan). The detailed methods were described previously [20]. The average baPWV from both left and right sides were used in the analysis (correlation between the right and left baPWVs: r2 = 0.925, p < 0.0001).
The assessment of dietary intake and physical activity level
Information on each participant's usual diet was obtained using both a 24-hour recall and a semi-quantitative food frequency questionnaire (SQFFQ), of which the validity had been previously tested [21]. We used the former to carry out analyses and the latter to check if the collected data was representative of the usual dietary pattern. All participants were given written and verbal instructions by a registered dietitian on completion of a 3-day (2 week days and 1 weekend) dietary record. Dietary energy values and nutrient content from the 3-day food records were calculated using the Computer Aided Nutritional Analysis Program (CAN-pro 3.0, Korean Nutrition Society, Seoul, Korea). Total energy expenditure (TEE) (kcal/day) was calculated from activity patterns (basal metabolic rate, 24 hour-physical activity, and specific dynamic action of food).
Statistical analysis
Statistical analyses were performed with Win SPSS ver. 20.0 (Statistical Package for the Social Science, SPSS Inc., Chicago, IL, USA). Differences in continuous variables among subgroups were tested with independent t-test or one-way ANOVA followed by Bonferroni correction for multiple comparisons to reduce the rate of false positive, and non-continuous variables were tested with χ2 test. A general linear model analysis (GLM, post-hoc multiple comparison tests) followed by Bonferroni correction was also performed to see the differences in the cardiovascular risk parameters according to major serum phospholipid FA composition with adjustment for confounding factors (i.e. age, anthropometric parameters, cigarette smoking, alcohol consumption, dietary intake etc.). Pearson correlation analysis was performed for the relationship among the variables. Multiple regression analysis was used to find the major determinants for arterial stiffness in metabolically healthy men. The skewed variables were log-transformed for statistical analysis. For descriptive purposes, the mean values are presented using untransformed values. Results are expressed as mean ± SE or percentages. A two-tailed value of p < 0.05 was considered statistically significant.
Go to :
RESULTS
General characteristics and basic biochemical parameters of study population
Table 1 presents demographic and metabolic characteristics of study population. Mean values of age, BMI, waist circumference, systolic BP, proportions of current smokers and current drinkers were significantly different between healthy and CAD patients. Regarding medications, most of CAD patients consumed anticoagulation drugs (99.1%) and antihypertensive drugs (92.7%). 70.9% of CAD patients consumed lipid-lowering drugs. None of them consumed antidiabetic drugs. Serum lipid profiles (triglyceride, HDL-cholesterol, total cholesterol, and LDL-cholesterol) were significantly different between the two subject groups. CAD men show significantly higher levels of insulin and HOMA-IR and lower levels of glucose and FFAs than healthy men, but all the values were in normal range. Serum creatine levels were statistically lower in CAD men than in healthy men, but the levels in both groups are in normal range. In addition, the values of another kidney function (BUN) and liver function (AST, ALT) markers were not significantly different between the two subject groups, and all the values are in normal range. Compared with CAD men, healthy men showed higher ratio of TEE to total calorie intake (TEE/TCI) and consumed higher percent energy intake from total fats and lower percent energy intake from total carbohydrates and proteins, and similar dietary polyunsaturated FAs to saturated FAs ratio (PUFA/SFA) (Table 1).
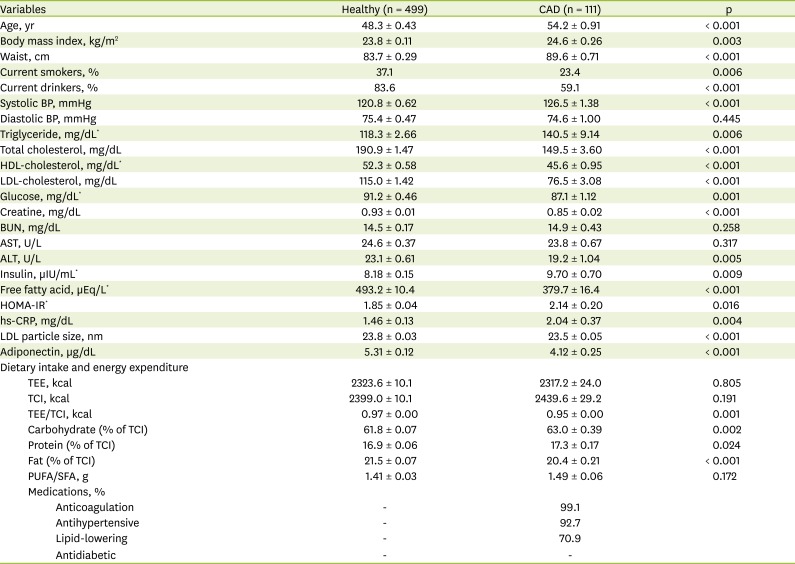
Table 1
Demographic and metabolic parameters of study population
Mean ± S.E or %.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BP, blood pressure; BUN, blood urea nitrogen; HOMA-IR, homeostasis model assessment of insulin resistance; hs-CRP, high sensitivity C-reactive protein; TEE, total energy expenditure; TCI, total caloric intake; PUFA, polyunsaturated fatty acid; SFA, saturated fatty acid.
*Tested after log transformed; tested by independent t-test (student t-test).
![]()
Differences in the proportions of serum phospholipid FAs between healthy men and CAD patients
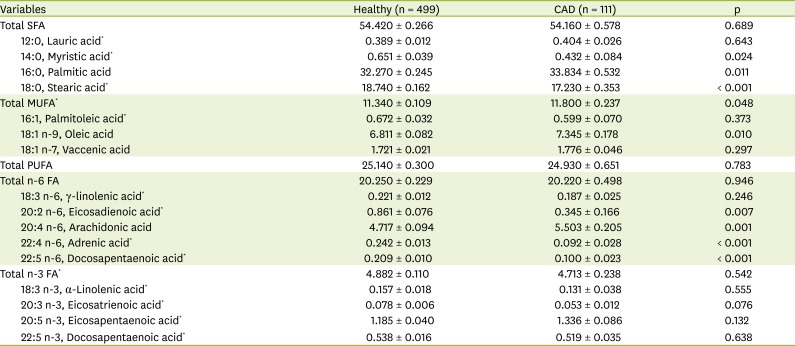
Figure 1 and Table 2 present serum phospholipid FA composition between healthy men and CAD patients. The values were adjusted for age, waist circumference, cigarette smoking, alcohol consumption, systolic blood pressure, HDL-cholesterol, TEE/TCI, dietary carbohydrates (% of total calorie intake), dietary fats (% of total calorie intake). The proportions of linoleic acid (LA, 18:2n-6) and DHA (22:6n-3) were significantly lower and that of dihomo-γ-linolenic acid (DGLA, 20:3n-6) and the ratio of n-6 PUFAs to n-3 PUFAs were significantly higher in CAD men than in healthy men (Figure 1). The proportions of myristic acid (14:0), palmitic acid (PA, 16:0), stearic acid (SA, 18:0), total monounsaturated FA, oleic acid (18:1n-9), eicosadienoic acid (20:2n-6), arachidonic acid (AA, 20:4n-6), adrenic acid (22:4n-6), docosapentaenoic aicd (20:5n-6) were significantly different between healthy and CAD men (Table 2).
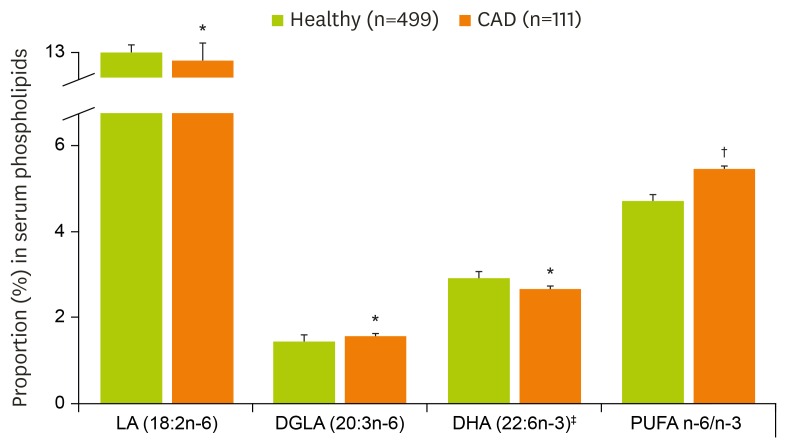 | Figure 1Proportions of serum phospholipid fatty acids between healthy men and CAD patients.
Mean ± S.E.
LA, linoleic acid; DGLA, dihomo-γ-linolenic acid; DHA, docosahexaenoic acid; PUFA, polyunsaturated fatty acid.
*p < 0.05 †p < 0.001 tested by general linear model (GLM) with adjustment for age, waist circumference, cigarette smoking, alcohol consumption, systolic blood pressure, HDL-cholesterol, total energy expenditure/total calorie intake, dietary carbohydrate (% of total calorie intake), dietary fat (% of total calorie intake); ‡Tested after log transformed.
|
Table 2
Differences in the proportions of serum phospholipid fatty acids between healthy men and CAD patients
Mean ± S.E.
p, p-value adjusted for age, waist circumference, cigarette smoking, alcohol consumption, systolic blood pressure, HDL-cholesterol, total energy expenditure/total calorie intake, dietary carbohydrate (% of total calorie intake), dietary fat (% of total calorie intake); FA, fatty acid; SFA, saturated fatty acid; MUFA, monounsturated fatty acid; PUFA, polyunsaturated fatty acid.
*Tested after log transformed; tested by general linear model (GLM) followed by bonferroni correction with adjustment.
![]()
Correlations among serum phospholipid FA composition
Pearson correlation analysis revealed that DHA (C22:6n-3) was highly correlated with many of LC-FAs in serum phospholipid FA composition in all the subject groups (whole subjects, healthy men and CAD patients respectively) : positively correlated with α-linolenic acid (ALNA, 18:3n-3, r = 0.138, p = 0.001; r = 0.102, p = 0.041; r = 0.369, p < 0.001, respectively), EPA (20:5n-3, r = 0.525, p < 0.0001; r = 0.434, p < 0.001; r = 0.830, p < 0.001, respectively), LA (18:2n-6, r = 0.448, p < 0.0001; r = 0.479, p <0.001; r = 0.317, p = 0.001, respectively), γ-linolenic acid (GLA, 18:3n-6, r = 0.191, p < 0.0001; r = 0.236, p < 0.001; r = 0.140, p = 0.042, respectively), DGLA (20:3n-6, r = 0.498, p < 0.0001; r = 0.537, p < 0.001; r = 0.361, p < 0.001, respectively), AA (20:4n-6, r = 0.684, p < 0.0001; r = 0.716, p < 0.001; r = 0.621, p < 0.001, respectively) and docosapentaenoic acid (DPA, 22:5n-6, r = 0.220, p < 0.0001; r = 0.214, p < 0.001; r = 0.320, p = 0.001, respectively), and negatively correlated with n-6 PUFAs/n-3 PUFAs (r = -0.716, p < 0.001; r = -0.695, p < 0.001; r = -0.851, p < 0.001, respectively).
The association of serum phospholipid DHA proportion with cardiovascular risk related parameters and arterial stiffness in metabolically healthy men
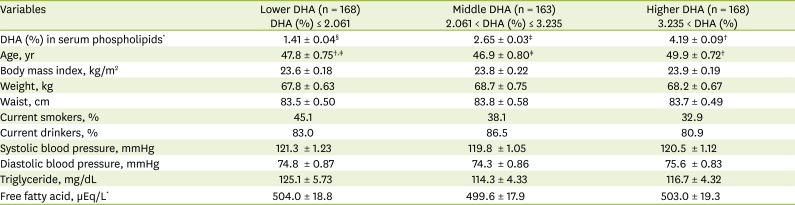
In order to investigate the relationship between serum phospholipid DHA and cardiovascular risk parameters including ba-PWV, healthy men were subdivided into three tertile groups according to the proportion (%) of DHA in serum phospholipids [lower-DHA group: DHA (%) ≤ 2.061; middle-DHA group: 2.061 < DHA (%) ≤ 3.235; and higher-DHA group: 3.235 < DHA (%)]. There were no significant differences in general and basic biochemical parameters except age among the DHA tertile groups (Table 3). After adjusted for age, cigarette smoking, alcohol consumption, and dietary intake, fasting glycemic index (glucose and HOMA-IR) were significantly higher in the lower-DHA group than in the higher-DHA group. On the other hand, plasma adiponectin levels were significantly lower in the lower-DHA group than in the higher-DHA group. Hs-CRP and ba-PWVs were significantly higher, but LDL particle size was lower in the lower-DHA group than in the higher-DHA group (Figure 2).
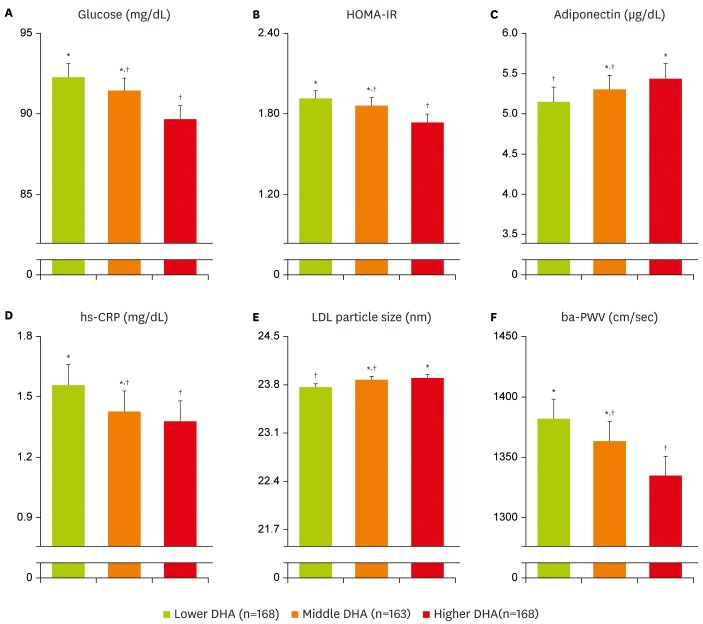 | Figure 2Association of serum phospholipid DHA proportion with cardiovascular risk related parameters and arterial stiffness in healthy men. (A) Glucose (mg/dL); (B) HOMA-IR; (C) Adiponectin (µg/dL); (D) hs-CRP (mg/dL); (E) LDL particle size (nm); (F) ba-PWV (cm/sec); (A-D, F) Tested after log transformed; Tested by general linear model (GLM) analysis followed by Bonferroni correction with adjustment for age, cigarette smoking, alcohol consumption, dietary intake.
Mean ± S.E.
DHA, docosahexaenoic acid; HOMA-IR, homeostasis model assessment of insulin resistance; hs-CRP, high sensitivity C-reactive protein; ba-PWV, brachial-ankle pulse wave velocity.
*,†Variables marked with the same mark indicates no significant difference. Healthy men were subdivided into three tertile groups according to the proportion (%) of DHA in serum phospholipids [lower DHA group: DHA (%) ≤ 2.061; middle DHA group: 2.061 < DHA (%) ≤ 3.235; and higher DHA group: 3.235 < DHA (%)].
|
Table 3
General characteristics and biochemical parameters according to the proportion (%) of DHA in serum phospholipids in healthy men
Mean ± S.E or %.
HOMA-IR, Homeostasis model assessment of insulin resistance; DHA, docosahexaenoic acid.
*Tested after log transformed; tested by one-way analysis of variance (ANOVA) with bonferroni correction; †,‡,§Sharing the same mark indicates no significant difference in each variable in the same row.
![]()
Association of DHA with arterial stiffness by multiple regression analysis
A multiple stepwise regression analysis was performed to identify the association of serum phospholipid DHA composition with arterial stiffness in metabolically healthy men. Input factors were age, waist circumference, BPs, triglyceride, HDL-cholesterol, LDL-cholesterol, HOMA-IR, LDL particle size, hs-CRP, plasma adiponectin, serum phospholipid DHA and basic parameters such as TEE/TCI, cigarette smoking and alcohol consumption which may be closely related with MS and CAD. Among the factors, serum phospholipid DHA was found one of main contributors to arterial stiffness [adjusted β-coefficients (β′) = -0.127, p = 0.006] together with age (β′ = 0.315, p < 0.001), systolic BP (β′ = 0.394, p < 0.001), triglyceride (β′ = 0.105, p = 0.023) in metabolically healthy men (r = 0.548, p = 0.023).
Go to :
DISCUSSION
This study presents that serum phospholipid DHA was significantly associated with the alterations of MS and cardiovascular risk related parameters, and arterial stiffness in metabolically healthy men. In our study, fasting glucose, HOMA-IR, hs-CRP and ba-PWVs were significantly higher and adiponectin and LDL particle size were significantly lower in the lower-DHA group than the higher-DHA group. Multiple stepwise regression analysis also revealed that serum phospholipid DHA was a protective contributor against arterial stiffness. These results may give evidences that serum phospholipid DHA plays a critical role in cardiometabolism and is inversely associated with arterial stiffness, a composite risk factor for early atherosclerosis [2223] in metabolically healthy people.
Jump et al. [24] reported that over 290 clinical and experimental studies have examined the impact of LC-PUFAs on cardiovascular risk (n = 110) including MS (n = 16), diabetes and obesity (n = 12), inflammation (n = 97), dyslipidemia (n = 55), and hypertension (n = 10). According to Vessby et al., [2] FA compositions in blood can be a marker for dietary fat composition and are associated with metabolic disorders: decreased LA and increased DGLA in blood phospholipids were associated with IR. In our current study, CAD patients showed lower proportions of LA, DHA and DPA, and higher proportions of DGLA and n-6/n-3 PUFAs than healthy men. The significances were maintained after the adjustment. Our previous study [3] also shows that serum phosopholipid FA compositions were significantly related to features of MS. Dietary n-3 PUFAs and fish consumption were reported to help depression of heart rate and reduction of sudden cardiac death in humans [2526], and to induce several genes related to cardiac cells which encode proteins involved in lipid transport and the metabolism [2728]. It may suggest that dietary n-3 PUFAs play a pathophysiologic role in the cardiometabolism including MS and myocardial dysfunctions [29].
Among the LC-PUFAs, DHA have been mainly investigated in the human and animal studies. Consumption of 0.7 g DHA/day for 3 months significantly increased DHA proportion in erythrocytes and reduced diastolic BP in middle-aged healthy subjects, but did not alter other inflammation and vascular function parameters [6]. In our previous study, DHA treatment significantly suppressed LPS-induced VSMC proliferation and inflammation by up-regulating the phosphorylation of ERK and p38, and inhibiting the translocation of NF-kB p65 from cytoplasm to nucleus in VSMCs [8]. In the spontaneously hypertensive rats, DHA supplementation significantly reduced BPs and vascular wall thicknesses of the coronary, thoracic, and abdominal aorta than control rats [30]. These results may support that DHA plays critical roles in cardiometabolism and has cardiovascular protective effect. However, most studies were performed in CAD patients or people with history and risk factor of CVD, and in the disease-based animal models. Only a few studies including cohort studies were done in healthy people.
The Atherosclerosis Risk in Communities Study performed in 1,908 middle aged healthy women reported that higher plasma phospholipid DHA can reduce the risk of heart failure [31]. Another cohort study performed in men aged 42 and more years old showed that serum DHA was associated with the risk of atrial fibrillation, a common cardiac arrhythmia [32]. Lindqvist et al. [33] showed that plasma phospholipid EPA was positively associated with HDL-cholesterol, total cholesterol, remained after adjustment for BP, and DHA was negatively related to serum endothelial markers (E-selectin, P-selectin), and positively with systolic BP. Recently, n-3 PUFA supplementation (4 g/day for 12 weeks) significantly increased EPA and DHA contents in erythrocytes and decreased blood triglyceride and carotid-femoral PWV in the healthy elderly, but the subjects numbers were so small (n = 12) [34]. In addition, fish consumption and coronary calcification had a weak inverse association in healthy women, but it did not reach the statistical significance [35]. Our current study investigated in metabolically healthy men (n = 499) showed that hs-CRP, and ba-PWV were significantly higher, and plasma adiponectin and LDL particle size were lower in the lower-DHA group than the higher-DHA group. These significances were still maintained after adjusted for confounding factors. These results may be explained that higher proportion of DHA in serum phospholipids suppressed the mRNA expression and production of several pro-inflammatory cytokines [36] which are closely associated with cardiometabolic risk parameters [49]. Many studies have reported the relationship between n3 LC-PUFAs, particularly DHA and glycemic status [637383940]. Minihane et al. [37] reported that diet containing high n6/n3 PUFAs significantly increased fasting insulin and HOMA-IR. Plasma DHA is negatively associated with HOMA-IR [3839] and effective on the prevention and treatment of IR in CAD patients with or without MS [38]. Recent animal study also showed that DHA consumption significantly reduced plasma glucose level and restored insulin sensitivity in skeletal muscle [40]. It was reported that DHA together with EPA altered membrane fluidity and interacted with peroxisome proliferator-activated receptor-gamma which regulates insulin sensitivity regulator, thereby improving glycemic status [41]. In our study, metabolically healthy men with higher DHA proportion showed lower levels of fasting glucose, insulin and HOMA-IR indicating fasting glycemic status than those with lower DHA proportion. From the previous and our current results, we may suggest that higher DHA in serum phospholipids has a beneficial effect on cardiometabolism and may reduce the cardiovascular risk even in metabolically healthy people. One limitation of the current study is that participants were only men aged 30-69, so the result may not be suitable for women. Future study needs to be done in both men and women.
Go to :
CONCLUSION
This study shows that lower proportion of DHA in serum phospholipids may be associated with increased cardiovascular risk and positively related with arterial stiffness in metabolically healthy men. It suggests that maintaining higher proportion of serum phospholipid DHA may be beneficial for reducing cardiovascular risk including arterial stiffness in healthy people.
Go to :
 XML Download
XML Download