

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Many studies have reported that cholesterol, triglycerides, and lipoproteins are involved in cancer incidence and severity. Moses et al. [1] reported that increased level of low density lipoprotein (LDL) was associated with a higher risk of prostate cancer in African American men. Tada et al. [2] found that high levels of serum triglycerides were positively correlated to cancer incidence in Japanese hypertriglyceridemia patients. Also increased levels of fasting glucose and c-peptide were observed with elevated body weight and increased plasma cholesterol in breast cancer patients at stage I-II [3]. Also a recent report from meta-analysis suggested that total serum cholesterol and high density lipoprotein cholesterol (HDL-C) were inversely associated with breast cancer risk [4].
Such dysregulated lipid status changes patterns of energy utilization, affects immune and inflammatory pathways, interacts with catecholamines and leads an alteration of body composition including fat and muscle amount [567]. Hence many cancer patients who sustain altered energy homeostasis (e.g. insulin resistance) in conjunction with uncontrolled blood lipid finally experience the accelerated loss of skeletal muscle mass [89101112]. For example Prado et al. [11] reported that decreased muscle mass and muscle strength (i.e. handgrip strength) were observed in male cancer patients with advanced lung or colon cancer. Gale et al. [12] suggested that less grip strength due to low muscle mass was associated with increased mortality from cancer in the analysis of the data from UK Department of Health and Social Security survey. Cancer patients with cachexia also showed catabolic conditions including elevated carbohydrate utilization, protein degradation and increased fat lipolysis, and these conditions led weight loss and were associated with increased morbidity and mortality of cancer patients [1314].
However it has been well suggested that elevated glucose level or longer duration of diabetes is associated with declines in skeletal muscle mass even in non-cancer subjects [8910]. Additionally metabolic changes observed in cancer patients are more complicate than those in patients only suffering from diabetic conditions [11131415]. Therefore, in cancer patients, diabetes or insulin resistance will not be the only factor affecting loss of skeletal muscle mass. Beside glycemic status, dyslipidemia and related complications observed in cancer patients were mostly explained in terms of decreased fat mass [131415] but their relationship with decreased skeletal muscle mass in cancer patients has not been well documented. Also muscle mass could be influenced by dietary factors or health conditions affecting lipid status specific to cancer hence the associations among altered metabolic conditions and muscle mass which differ from non-cancer subjects need to be explored in cancer patients. Based on such research gaps this study was conducted to investigate the relationship of serum lipids with relative lean body mass in cancer patients without a diagnosed diabetes by utilizing the Korean National Health and Nutrition Examination Survey (KNHANES) data from 2008-2011.
Materials and Methods
Study participants
KNHANES used a stratified multistage probability design to provide nationally representative estimates of Korean population [1617]. The data from KNHANES 2008-2011 containing the assessment of dual-energy X-ray absorptiometry (DXA) in participants were used. Of 28071 potential participants aged ≥ 30 years, 230 participants who were diagnosed cancer (stomach, colorectal, liver, lung, breast, ovary) were included in the study. Participants with known history of diabetes and/or use of insulin therapy were excluded and further participants who had incomplete lab data were excluded. Finally the data of 179 subjects were analyzed for the present study. Control subjects were also used for differentiating the health characteristics of cancer patients from subjects without cancer before exploring the possible variables associated with lean body mass in cancer patients. Total of 19172 participants who were older than 30 years, has no history of diabetes or insulin use but never been diagnosed cancer were used as control subjects only for comparing general health or diet characteristic of cancer patients to that of non-cancer subjects. Since the number of cancer subjects from the data of this complex sampling design was not large enough to be matched by the data from non-cancer subjects the comparison between cancer patients and control group was performed on the raw data without stratification or adjustment. KNHANES was approved by the Institutional Review Board of the Korea Center for Disease Control and Prevention (IRB No. 2008-04EXP-01-C, 2009-01CON-03-2C, 2010-02CON-21, 2011-02CON-06-C).
Assessment of lean body mass
The whole body DXA examination in KNHANES was acquired according to the manufacture's instruction on a Discovery-W fan-beam densitometer (Hologic Inc., Bedford, MA, USA). All subjects were asked to take off all accessories which could interfere with the DXA examination. The coefficient of variation (CV) of bone mineral density (BMD) measurement of lumbar spine (L1-L4), femoral neck and whole femur were less than 1.9%, 2.5% and 1.8%, respectively [16]. Additional information for the precision of the DXA instrument used or calibration in the KNHANES study was reported previously [161718]. Total lean body mass was obtained from all anatomical regions of skeletal muscle. Appendicular lean body mass was obtained from combined lean body masses in the right and left arms and legs [16]. All obtained values of lean body mass (kg) were divided by total body weight (kg) and multiplied by 100% to provide standardized estimates of percent lean body mass which could be better account for lean mass relative to body size as reported previously [19].
Measurement of covariates
Height was measured by a balanced beam scale (Seca 225, Seca, Germany) and body weight was measured using a digital electronic scale (GL-6000-20, G-tech, Korea). Body mass index (BMI) was calculated as the weight (kg) to the square of height (m2). Blood samples were obtained from a cephalic vein of the study subjects. Fasting plasma glucose, hemoglobin A1c (HbA1c), blood urea nitrogen (BUN), total cholesterol (total-C), triglyceride and HDL-C levels were measured using a Hitachi 7600 chemistry analyzer (Hitachi, Tokyo, Japan).
Participants were asked if they did physical activity designed for enhancement of muscle strength such as push-ups, situps, lifting weights or the horizontal bar in the last week. Status of smoking was categorized either a smoker: a person who had smoked more than five packs of cigarettes in the past, or a non-smoker: a person who had no history of smoking. Status of alcohol consumption was defined based on whether a person currently drinks alcohol more than one time per month (drinkers) or not (non-drinkers).
Nutrient intakes such as carbohydrate, lipid and proteins were assessed with a 24-hour dietary recall questionnaire administered by a trained survey researcher. The results from a 24-hour recall were calculated using the Food Composition tables developed by the National Rural Resources Development Institute (7th revision) [20].
History of comorbidities including arthritis, cardiovascular disease (CVD), asthma, hypertension or chronic obstructive pulmonary disease (COPD) was self-reported by study subjects.
Statistical analysis
All statistical analyses were conducted using SAS software version 9.3 (SAS Institute Inc., Cary, NC, USA). Values of demographic and health-related variables were expressed as mean and standard error for continuous variables or, number of frequency and percentages for categorical variables. For the comparison with non-cancer healthy subjects the t-test was used for continuous variables and the chi-square test for categorical variables. Pearson's correlation test was used to explore simple correlation of percent lean body mass and health related continuous variables. The 'domain' statement was used to provide less-biased estimates for subgroup analysis in the survey data. Before selecting variables for linear regression model collinearity was checked for each independent variable related to lean body mass. Linear regression models were created and tested to characterize the association of percent lean body mass and variables related to energy metabolism in cancer patients. Key covariates accounted in regression models were as follows; Model I: adjusted for age, sex, physical activity, smoking, height, serum total-C, serum total triglyceride and fasting glucose, Model II: Model I + energy intake and Model III: Model II + comorbidities which are the presence of CVD (n = 22), arthritis (n = 3), COPD (n = 15), asthma (n = 4) or hypertension (n = 50). These covariates were chosen as potential confounders of the association between hyperglycemia/hypercholesterolemia and muscle mass. Since lean body mass was initially standardized to body weight, the height was adjusted for the analysis. With these characterized models further analyses were performed to estimate beta coefficient, 95% CIs for percent lean body mass by quartiles of serum total-C, taking the lowest quartiles group as the reference group, in male and female subjects separately. Quartiles of serum total-C were categorized for male as follows: 1st quartile (Q1): total-C < 161, 2nd quartile (Q2): 161 ≤ total-C < 180, 3rd quartile (Q3): 180 ≤ total-C < 211, 4th quartile (Q4): total-C ≥ 211, for female as follows: Q1 total-C < 145, Q2:145 ≤ total-C < 182.5, Q3:182.5 ≤ total-C < 208, Q4:total-C ≥ 208, and for whole subjects (both male and female) as follows: Q1:total-C < 156, Q2:156 ≤ total-C < 180, Q3:180 ≤ total-C < 209, Q4:total-C ≥ 209. A p value of less than 0.05 was considered statistically significant.
Results
Initially data of skeletal muscle mass and related outcomes were compared between cancer patients and non-diabetic subjects without cancer (Table1). The mean age of cancer patients was higher than that of healthy non-cancer subjects (p < 0.0001). The body weight and BMI were not different betwe en two groups but the lean body mass (p = 0.0004) and appendicular lean body mass (p < 0.0001) were significantly low in cancer patients. The level of HbA1c, fasting glucose, total-C, HDL-C, TG and BUN was not different between cancer patients and non-cancer subjects. Also overall nutrient intake except for carbohydrate consumption was lower in cancer patients compared to non-cancer subjects. The number of subjects who performed physical activity designed for muscle enhancement was not different between two groups. The frequency ratio of the presence of alcohol drinking and the history of cigarette smoking in cancer patients were less than non-cancer subjects (p < 0.0001 for both parameters).
Table 2 shows results from simple correlation test between lean body mass and variables which could affect skeletal muscle before any adjustment was made for the weighted data. The simple correlation analysis revealed that the height, the level of BUN, the intake of energy and nutrients (protein, carbohydrate, fat) were positively correlated with percent lean body mass in both cancer patients and non-cancer subjects. The lean body mass and the level of total-C was negatively correlated both in cancer patients (r = -0.2765, p < 0.0001) and in non-cancer subjects (r = -0.1710, p < 0.0001). Correlation between lean body mass and age was positive in cancer patients (p = 0.0002) while negative correlation was observed in non-cancer subjects.
Three linear regression models for cancer patients were developed using the variables which showed relatively high level of correlation coefficient with lean body mass in order to explore the main predictor of lean body mass in cancer patients (Table 3). First linear model (Model I) demonstrated that sex, physical activity and total-C were significantly associated with lean body mass. However weak or no association was observed between lean body mass and fasting glucose (p = 0.0948) or serum triglycerides (p = 0.2692). After nutrient intakes (energy, carbohydrate, protein and fat intake) were adjusted (Model II) the energy and carbohydrate intake were significantly associated with lean body mass while the direction of these associations were opposite each other. The association of lean body mass with sex, physical activity, total-C, total energy intake and carbohydrate intake was still significant after accounting for diabetes-related comorbidities (Model III). When the use of cholesterol lowering drugs (daily use) was incorporated in the model the association between lean body mass and total-C or other variables were not affected. (data not shown). However the effect of total energy intake and carbohydrate on the lean body mass was disappeared after adjusting for HDL-C (data not shown). Also same regression models were tested for appendicular lean body mass (Table 3) and the association between total-C and appendicular lean body mass was same as seen in the models for total lean body mass with higher R2 value for all three regression models (R2 = 0.6521, 0.6676, and 0.6712 for Model I, II, and III, respectively).
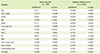
Since sex, physical activity and the total-C were significantly associated with percent lean body mass at the total body including appendicular sites in all linear regression models, the relationship was further analyzed within same sex by quartiles of total-C (Table 4). Male cancer patients were getting lower lean body mass compared to reference (the lowest quartile of total-C) by increased quartiles of total-C in all three regression models but the trend was not significant. In female cancer patients only the highest quartile (total-C ≥ 208 mg/dL) of total-C had significantly lower percent lean body mass compared to reference in models adjusted for physical activity (Model I), the nutrient intake (Model II) and in fully adjusted model (Model III). For whole subjects including both male and female all three higher quartiles of total-C versus reference were also associated with significantly lower lean body mass in all three tested regression models. When these regression models were tested (Table 4) for appendicular lean body mass male cancer patients showed significantly lower lean body mass compared to reference in the highest quartile (total-C ≥ 211 mg/dL) of total-C (p < 0.0001). In whole subjects only the highest quartile (total-C ≥ 209 mg/dL) of total-C had significantly lower appendicular lean body mass compared to reference in all three regression models (p < 0.05).
Discussion
The loss of muscle mass is associated with decreased muscle strength, consequently, and negatively impacting functional muscle capacity, and leads increased mortality [122122]. Also subjects with sarcopenia have higher risk of infection than older patients with a normal skeletal muscle mass [2324]. Cancer patients usually experience progressive weight loss accompanied with reduction of lean body mass which is responsible for a poor quality of life and poor response to chemotherapy with a shorter survival time than in cancer patients without weight loss [2425]. In this study percent lean body mass was relatively low in cancer patients compared to non-cancer subjects without significant difference in BMI or body weights indicating the change of body composition toward a decrease of skeletal muscle mass in cancer patients. Also the results showed that sex and physical activity were associated with lean body mass in cancer patients and were consistent with well-established findings from previous studies which supported the difference of skeletal muscle mass by sex and the response of skeletal muscle to exercise or the level of physical activity in normal healthy subjects [2627]. On the other hand, the muscle loss by aging has been well evidenced by past studies [232427] but aging induced muscle loss was not observed in cancer patients of this study and rather positive correlation was observed between muscle mass and aging. These results implicate that decreased muscle mass in cancer patients is likely due to metabolic alteration specific to cancer at the age of their illness and is different than gradual downfall of muscle mass by aging process.
Of many other parameters which were found to be correlated with skeletal muscle mass in this study total-C was an only serum factor showing consistently negative association with lean body mass in cancer patients. Serum cholesterol has been reported to be responsible for incidence or progression of cardiovascular diseases and metabolic disease such as cancer [282930]. Studies reported that men with low serum cholesterol had a lower risk of prostate cancer [28] and the long-term use of cholesterol lowering drugs attenuated the progression of prostate cancer [29]. Also the low level of serum total-C was positively associated with the incidence of high grade prostate cancer and the risk was higher in subjects with higher BMI [30]. In regards to the role of cholesterol on muscle mass, so far, there have been no human studies which specify the role of cholesterol in muscle mass of cancer patients. However, numerous experimental studies suggest that the increase of serum total-C is attributed in reduced lipoprotein lipase (LPL) activity in cancer [313233] which mediates decreased cellular uptake of fatty acids by hydrolysis of lipoproteins and is associated with hypertriglyceridemia, and hyperlipidemia accompanied with weight loss [34]. Also lower levels of serum TG, glycerol and free fatty acids have been observed in cancer patients with cachectic conditions [3334] though the LPL activity was not determined in these studies. In our current study two higher quartiles of serum total-C were negatively associated with lean body mass in the regression models with quartile level of total-C for estimation of skeletal muscle mass of cancer patients. This result suggests that uncontrolled catabolic conditions of cancer patients underlie both decreased lean body mass but increased serum level of cholesterol.
In this study the pattern of relationship between lean body mass and quartile of total-C was different between male and female cancer patients. Though the results were not significant the trend that proportional decline in lean body mass by the level of serum total-C was more noticeable in male subjects than female subjects who showed dramatic downfall of muscle mass only in bearing with highest level of total-C (more than 208 mg/dL). In appendicular lean body mass, however, a subtle change of muscle mass was observed in male subjects and whole subjects in the other two quartile levels of total-C which considered normal range of serum total-C value. There is no obvious reason to explain differences between male and female but also it's difficult to judge whether such difference is reliable in limited number of subjects within each quartile group. Nevertheless the differences in the amount and distribution of skeletal muscle between men and women could be a part of this result. For example skeletal muscle in lower limb took part greater proportion of appendicular lean body mass in male than in female and then muscle strength (i.e., handgrip strength) was associated with less amount of appendicular lean body mass in women [35]. Furthermore, since sex-related differences exist in the rate of weight loss [2627], the response of skeletal muscle to substances from blood circulation (e.g., steroid hormone, systemic lipid or cytokines) or nutrient changes might be different between male and female.
In this study energy or nutrient consumption was associated with muscle mass but when other disease factors were adjusted the effect of dietary factors were disappeared. Since 24h recall data from this cross-sectional KNHANES did not precisely reflect nutrient consumption, further incorporation of data from food frequency questionnaire (FFQ) will give more reliable information about the nutritional status of the subjects. However, results from regression analyses in this study are supported by previous findings that the dietary factor is not the only factor accounting for muscle loss [363738]. There are numerous evidences that, rather than change of nutrient intake, more of systemic inflammation induced by tumor cell derived cytokines disturb metabolic balance under cachexia [363738]. In addition, studies with cancer patients suffering from muscle loss reported that metabolic alterations including elevated carbohydrate utilization and decreased fat stores in cancer patients were mainly due to increased lipolysis rather than reduced lipid biogenesis [3233]. Also if nutrient supply is low then this would be represented by blood parameters but, in this study, the level of blood glucose or serum triglycerides was not different between cancer patients and non-cancer subjects and their associations with lean body mass in regression models were not significant. Furthermore, incorporation of the parameter which indicate the use of lipids lowering drugs did not affect the power of the model (R2 value in model III, 0.5964 vs. 0.5967) and did not change the value or significance of the beta coefficient for selected variables in the model (data not shown). Taken together these data indicate that loss of skeletal muscle mass in cancer patient is related to the dysregulated metabolic changes more likely than supply aspect.
The study also has limitations. First, we cannot conclude that all cancer subjects in this KNHANES study were experiencing muscle loss but also cannot generalize the finding of this study as the general phenomenon of cancer patients. However, many cancer patients (more than 50%) experience muscle wasting [353940] and patients with weight loss, even at 15% loss, are related to the reduced survival time of cancer patients due to the loss of respiratory function or circulation capacity [40]. Second, the number of cancer subjects in KNHANES data was small and the data were analyzed from mixed subjects who suffered from various types of cancer so the findings from such small and mixed pool may hardly reflect common features of cancer patients. In spite of weak regression coefficients the association between total-C and total lean body mass was consistent throughout all possible regression models in this study. Hence, the data from this study could provide applicable foundation for future study of metabolic characteristics and skeletal muscle or muscle function only specific to cancer patients. Concerning several beneficial roles of skeletal muscle in energy metabolism, further identification of mechanisms and mediators of skeletal muscle loss under cancer illness would help developing early nutrition interventions to prevent further muscle wasting and to improve survival in cancer patients. Last, a type of cancer, stage of cancer should be accounted for the future analysis.
Conclusion
This study was performed to explore the independent relationship of serum lipids with relative lean body mass in nondiabetic cancer patients by utilizing KNHANES data from 2008-2011. In Korean cancer patients higher level of serum total-C was negatively associated with total and appendicular lean body mass (p < 0.0001) after adjusting key covariates (sex, age, physical activity, comorbidity, and energy intake etc.) while the correlation or the association of the other blood parameter (fasting glucose, HbA1c, BUN, and TG) with lean body mass were not statistically significant. However the effect of total-C was consistently significant in various linear regression models for estimation of skeletal muscle mass in cancer patients while the effects of nutrient consumption on lean body mass were disappeared after adjusting comorbidities of cancer patients. When linear regression models were tested with a quartile of total-C the higher quartile of total-C had lower lean body mass than reference quartile within male and female group of cancer patients and in whole subjects. These data suggest that the level of cholesterol can be the potential indicator of the loss of skeletal muscle in cancer patients and the data can be referred to a nutrition care of cancer patients with cachexia or parenteral/enteral nutrition. Causality of the findings in this study needs to be investigated in longitudinal study with large pool of subjects and the type or stage of cancer should be specified in future study.



 XML Download
XML Download