

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Diabetes mellitus (DM) is not only an important and dependent risk factor, but also a predictor of adverse outcomes for cardio-cerebrovascular diseases (i.e. coronary heart disease, stroke, heart failure, and peripheral artery disease) [1,2,3]. Glycemic measures, such as fasting glucose, 2-hour glucose, and glycated hemoglobin (HgbA1C) have been recommended for the diagnosis of diabetes and glycemic control [4,5]. Classically, fasting glucose is considered the standard measure used for the diagnosis of diabetes, and HgbA1C is recommended for the determination of long-term glycemic control in patients with DM [4,5]. In diabetic patients, increased values of HgbA1C were associated with a marked excess in cardiovascular disease (CVD) risk independent of classical CVD risk factors [6,7]. However, increased levels of HgbA1C and fasting glucose were associated with coronary artery calcification in general population without DM or cardio-cerebrovascular diseases [8].
Recently, evidences from epidemiological and clinical studies have reported that as compared to fasting blood glucose, HgbA1C was more strongly associated with the risk of atherosclerosis and CVD [9,10]. According to the earlier cross-sectional investigation within the Framingham Heart Study, normoglycemic HgbA1C (< 6.5%) may serve as a useful CVD risk marker in non-diabetic individuals [11]. Subsequent prospective studies also reported the associations of high-normal HgbA1C values with the increased risk of incident cardio-cerebrovascular diseases [3,9,10,12,13], indicating an independent relationship of HgbA1C with CVD risk in non-diabetic individuals [3,8,12,13]. In a study of 307 non-diabetic, stroke Korean male adults, the highest quartile of HgbA1C in normal range was significantly associated with the increased risk for ischemic stroke as compared to the lowest HgbA1C (≤ 5.3%) [3].
However, there were few studies comparing HgbA1C and fasting glucose as a marker reflecting cardiometabolic risk in non-diabetic Korean women. Therefore, this study aimed to investigate if HgbA1C as compared to fasting blood glucose is a better marker for reflecting cardiometabolic risk in nondiabetic Korean women.
Materials and Methods
Study participant and design
Study participant (women) were recruited from the Health Promotion Center at Dong-A University Hospital between Januarys 2014 and March 2014. They do not have any history of diseases. Exclusion criteria were following: 1) patients diagnosed for diabetic mellitus and stroke; 2) any diagnosis of vascular disease, cancer (clinically or by anamnesis), renal disease, liver disease, thyroid disease, and acute or chronic inflammatory disease. Totally ninety-one subjects (n = 91) were recruited and agreed to the participation consent form. The written informed consent proved before participation was approved by the Institutional Review Board of Dong-a University.
Anthropometric parameters, blood pressure and blood collection
Body mass index (BMI, kg/m2) was calculated using body height and weight. Blood pressure was measured in the arm of seated patients with an automatic blood pressure monitor (HEM-7220, OMRON, Matsusaka, Japan) after a rest. After overnight fasting, venous blood samples were collected in ethylenediaminetetraacetic acid (EDTA) - treated and plain tubes, separated into plasma and serum, and then stored at -80℃ until analysis.
Serum lipid profile
Fasting total cholesterol and triglyceride levels were measured using commercially available kits on a Hitachi 7150 Autoanalyzer (Hitachi Ltd., Tokyo, Japan). After precipitation of serum chylomicrons with dextran sulfate magnesium, the concentrations of low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol in the supernatants were enzymatically measured.
Fasting glucose, glycated hemoglobin (HgbA1C) and liver function
Fasting glucose levels were measured using a glucose oxidase method with a Beckman Glucose Analyzer (Beckman Instruments, Irvine, CA, USA). Glycated hemoglobin (HgbA1C) was measured using Variant II Turbo HgbA1C kit-2.0 (Bio-Rad, Hercules, CA, USA) on Variant analyzer (Variant II TURBO, Bio-Rad, Hercules, CA, USA). Serum aspartate aminotransferase (AST), alanine aminotransferase (ALT) were measured by a Modified IFCC UV method.
Data analysis
Statistical analyses were performed using SPSS version 21.0 for Windows (SPSS Inc., Chicago, IL, USA). Spearman and partial correlation analyses were performed for the relationships of fasting glucose or HgbA1C with basic and biochemical parameters. Skewed variables were log transformed for statistical analysis. For descriptive purposes, mean values were presented using untransformed values. Results were expressed as means ± SE or percentages. A two-tailed p value < 0.05 was considered statistically significant.
Results
General characteristics and biochemical parameters of study subjects
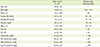
Table 1 shows general characteristics and baseline parameters such as age, body mass index (BMI), waist circumference, blood pressures, liver functions, fasting glucose, HgbA1C and lipid profiles of entire study subjects. Mean value of fasting glucose and HgbA1C were in the normal ranges (89.1 ± 1.19 and 5.26 ± 0.04, respectively).
Relationships of fasting glucose or HgbA1C with blood pressure and liver function markers
Both fasting glucose and HgbA1C were positively correlated with age (r = 0.202, p = 0.008; r = 0.221, p = 0.035, respectively), waist circumference (r0 = 0.296, p = 0.005; r0 = 0.304, p = 0.004, respectively). As shown in Figure 1, diastolic blood pressure (DBP) was positively correlated with fasting glucose (r0 = 0.206, p = 0.050) and HgbA1C (r0 = 0.225, p = 0.032). AST and ALT, the liver function markers, were also positively correlated with fasting glucose (r0 = 0.237, p = 0.024; r0 = 0.296, p = 0.004, respectively) and HgbA1C (r0 = 0.368, p < 0.0001; r0 = 0.356, p = 0.001, respectively). When adjusted for age and BMI, significant relationships of DBP (r1 = 0.190, p = 0.049), AST (r1 = 0.262, p = 0.0018), ALT (r1 = 0.277, p = 0.012) with HgbA1C were still retained, but those with fasting glucose disappeared.
Relationships of fasting glucose or HgbA1C with fasting lipid profiles
Figure 2 presents relationship between lipid profiles and fasting glucose or HgbA1C. Both fasting glucose and HgbA1C were positively correlated with triglyceride (r0 = 0.372, p < 0.001; r0 = 0.208, p = 0.008, respectively), LDL-cholesterol (r0 = 0.315, p = 0.002; r0 = 0.373, p < 0.0001, respectively) and total cholesterol (r0 = 0.310, p = 0.003; r0 = 0.284, p = 0.006, respectively), and negatively correlated with HDL-cholesterol (r0 = -0.287, p = 0.006; r0 = -0.261, p = 0.012, respectively). Further adjustment for age and BMI still maintained the significant positive correlation of fasting glucose or HgbA1C with total cholesterol (r1 = 0.232, p = 0.038; r1 = 0.265, p = 0.017, respectively) and LDL-cholesterol (r1 = 0.247, p = 0.026; r1 = 0.400, p < 0.0001, respectively), but not with triglyceride (r1 = 0.117, p = 0.115; r1 = 0.181, p = 0.115, respectively). In addition, the negative relationship between HDL-cholesterol with HgbA1C (r1 = -0.202, p = 0.029) were still maintained but those with fasting glucose disappeared (Figure 2).
Discussion
The aim of this study was to investigate if HgbA1C as compared to fasting blood glucose is better for reflecting cardiometabolic risk in non-diabetic Korean women. Study result shows that both fasting glucose and HgbA1C were negatively correlated with HDL-cholesterol and positively correlated with DBP, AST, ALT, triglyceride, LDL-cholesterol and total cholesterol. When adjusted for age and BMI, significant relationships of DBP, AST, ALT, and HDL-cholesterol with HgbA1C were still maintained, but those with fasting glucose disappeared. In addition, the adjusted relationships of LDL-cholesterol and total cholesterol with HgbA1C were much greater than those with fasting glucose. These results may suggest that HgbA1C as compared to fasting glucose is more sensitive for reflecting cardiometabolic risk in non-diabetic Korean women, thereby being a more predictable parameter for cardiometabolic risk in non-diabetic condition.
Many of epidemiological and clinical studies have reported increased lipid abnormalities in uncontrolled diabetic individuals, which contribute to higher rates of CVD [9,10]. Therefore, lipid management aimed at lowering LDL cholesterol and triglycerides, and raising HDL cholesterol has been applied to reduce CVD risk and mortality in type 2 diabetes [14]. As reported, insulin is a potent anti-lipolytic hormone and restrains lypolysis (release of free fatty acids, FFA) from the adipocytes by inhibiting the enzyme lipase. Fat cells in patients with type 2 DM or with metabolic syndrome (MetS, i.e. impaired glucose status, dyslipidemia, higher blood pressure, obesity) are resistant to the inhibitory effect of insulin on lipolysis [15]. This leads to a release of large amounts of FFA into the blood, thereby the increased FFAs producing lipid abnormalities mainly such as increased triglycerides and decreased HDL which causes atherogenic dyslipidemia [16]. In our study, both fasting glucose and HgbA1C were negatively correlated with HDL-cholesterol and positively correlated with triglyceride, LDL-cholesterol and total cholesterol. When adjusted for age and BMI, the significant relationships of LDL-cholesterol and total cholesterol with fasting glucose or HgbA1C were still retained, but the relationship between HDL-cholesterol and fasting glucose disappeared. This may indicate that HgbA1C as compared to fasting glucose is more sensitive to reflect cardiometabolic risk in non-diabetic Korean women.
In our study, DBP was positively associated with HgbA1C and the relationship was still maintained after adjusted for age and BMI. It may be partly explained by the report that dyslipidemia and hyerpinsulinemia in DM are associated with vascular dysfunction (i.e. increased vascular smooth muscle cell proliferation, arterial stiffness and vascular tone, and decreased vasodilation) and sodium retention which cause hypertension [17].
In addition, our study shows that AST and ALT the liver function markers were significantly associated with fasting glucose and HgbA1C levels. Particularly, the relationships with HgbA1C were still retained after adjusted for age and BMI. Our result is partly in accordance with the report by Fraser et al. [18] and Kim et al. [19]: when ALT and gamma-glutamyltransferase (GGT) levels were subdivided into tertiles, the levels of fasting insulin, fasting glucose and HgbA1C were higher in the highest terile of ATL and GGT levels in both non-diabetic and diabetic, although the associations of ALT and GGT with fasting glucose and HgbA1C were stronger in women with DM compared to those without DM [18]. Kim et al. also reported that the significant association between serum levels of GGT and the presence of the MetS even after adjusted for the presence of fatty liver, suggests that another mechanism governs the relationship between serum GGT and MetS [19].
This study has limitations. First, it did not allow for the sequential assessment of a direct association between fasting glucose or HgbA1C and cardiometabolic risk in non-diabetic individuals, because the exposure and outcome data were collected at a single time point. Second, only age and BMI (one of representative parameters for degree of obesity) were used as the adjustment parameters in partial correlation analysis. If other confounding factors (i.e. body fat percentage or distribution etc.) were additionally measured and adjusted, the conclusion would be more strongly supported.


 XML Download
XML Download