

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Prevalence of chronic illnesses is increasing due to rapid economic development, undesirable lifestyle and diet, and the increase of elderly population [1,2]. Particularly, a cardiovascular disease is one of the top three causes of death around the world and induces significant economic burden [3,4]. In South Korea, prevalence of dyslipidemia is also increasing and contributes to growing of death and morbidity rate in patients with cardiovascular diseases [5,6]. Various factors such as age, physical activity, obesity, heredity and stresses are affecting the d e velopment of dyslipidemia [7] and, especially, a diet is the most influencing factor to dyslipidemia [8]. Hence a certain but official format of dietary guidelines is necessary and become important component in effective management and prevention of dyslipidemia [9]. Korean Society of Lipidology and Atherosclerosis proposed a modified and supplemented dyslipidemia treatment guideline in 2009. The guideline recommends maintaining normal weight; limiting cholesterol intake to 200 mg per day as suggested by national cholesterol education program adult treatment panel III (NCEP-ATP III); limiting saturated fatty acids to 7% of the total energy intake, as the intake of animal lipids is increasing; limiting trans fatty acids less than 1% of the total energy intake recommend by world health organization (WHO); polyunsaturated fatty acid to 10% of the total energy intake, soluble dietary fiber to 10-25 g/d; carbohydrate to 60% of the total energy intake; and alcohol less than two glasses per day [10]. Furthermore, relevant guidelines were announced in USA and European countries and the correlation between dyslipidemia and diet were emphasized in their announcement [11,12].
In South Korea, for systematic and intensified dietary management in clinics and hospitals, the Korean goverment legislated certification system for government certified clinical dietitians in 2010 and began this certification system in 2012 to foster government-certified clinical dietitians who will perform nutrition assessment, nutrition consultation, and nutrition monitoring and evaluation [13]. Professional clinical nutrition service has been reported to have positive effects on reducing length of stay (LOS) and medical costs of patients [14,15,16], and Korean medical staff of the clinical nutrition services for disease management are always in high demands in Korea [17]. In the U.S., joint commission on accreditation of health organization (JCAHO) and academy of nutrition & dietetics (AND, former American dietetic association) participated in developing nutrition care standard for clinical dietitians in planning of diet therapy [18] and AND proposed standards of practice (SOP) and standard of professional performance (SOPP) for clinical dietitians [19,20]. Although Korean hospitals and clinics introduced the concept of nutrition care process (NCP) for standardizing the process of nutrition management by clinical dietitians, actual NCP application cases in the field are very limited so far. Also, even though several researched investigated job characteristics and level of job-satisfactions of dietitians in healthcare centers, schools and hospitals there are no relevant job standard to evaluate job performance or properties of dietitians and the proportion of clinical nutrinutrition tasks in their daily duties is very low [21,22,23,24,25]. Recently, developing a curriculum (DACUM) for defining the job of clinical dietitians at hospitals and standardizing the job based on job description was attempted and devleoped by nutrition experts. However, only a few researches has been conducted regarding job analysis and standardization of tasks for clinical dietitians according to a type of diseases. Therefore, in this study, the job of clinical dietitians who are involved nutrition management of dyslipidemia patients will be analyzed and job standards developed, in order to effectively manage and treat patients with dyslipidemia.
Materials and Methods
Current status and practice of clinical nutrition services
This study was approved by institutional review board (IRB, approval no.: YUHS01-13-003) of Yeungnam university. A survey was conducted on general status of hospital, the number of hospital beds (permitted beds, adjustable beds), clinical dietitian workforce, practice and result of nutrition education and consultation programs, and other questions related to dyslipidemia management by post-mail and email with clinical dietitians at medium and large hospitals with 300 or more beds in Korea from March 2014 to April 2014. Among 239 hospitals, questionnaire was collected from 104 hospitals (39 tertiary hospitals, 59 general hospitals, 6 hospitals), and that was 43.5% answering rate.
Job analysis and job standards development
In order to develop job standards to standardize the job of clinical nutrition service for dyslipidemia, a DACUM committee was made up of 17 members including clinical dietitians. DACUM is a method to extract task and task elements of clinical dietitians who provide the service to dyslipidemia patients and through this process DACUM creates a relevant job list. The DACUM committee workshop, first, defined the job of clinical dietitians for dyslipidemia and created competency standards based on characteristics of dyslipidemia. The job standard was composed of job elements of basic nutrition care services that clinical dietitian performed and recommended nutrition services specific for dyslipidemia patients. Details of recommended services were added, and, after several meetings, a draft of job standards based on NCP and practice was drawn. Later, the job standards were modified and supplemented based on advice and review of relevant institutes and experts.
Field application evaluation
For field application evaluation, 10 medical institutions among those with most trainings on dyslipidemia were selected based on the size and region of institution. The survey included job performance, difficulty, and job standard form evaluation, and, for job performance, performance of each task element was studied at each medical institution based on medical records of three cases of clinical nutrition service. Also, task difficulty was recorded based on 'basic service' and 'recommended service' according to practical experience of the subjects, while the job standards form was evaluated by having the subjects write their opinion on changes that need to be made.
Statistical analysis
All statistical analyses were based on SPSS 21.0 (IBM Corp., NY, USA), and general information of the hospitals was expressed in frequency (percentage) and average ± standard deviation. Education fee and reason for not receiving education fee were examined using multiple responses. ANOVA was used to compare in dyslipidemia nutrition education costs between different types of education. For an inter-group analysis, a post-hoc analysis was performed with Scheffe test. Statistical significance was set at p < 0.05.
Results
Practice of clinical nutrition service for dyslipidemia
General status of the hospitals
Of the 104 hospitals that participated in this study, 39 (37.5%) were tertiary hospitals, 59 (56.7%) general hospitals, and 6 (5.8%) hospitals. The number of permitted beds was highest in tertiary hospitals, average 985, followed by general hospitals, 599, and hospitals, 393. Also, 69.2% of tertiary hospitals, 56.9% of general hospitals, and 16.7% of hospitals had a separate nutrition education rooms (Table 1).
Current status of clinical nutrition service for dyslipidemia
Table 2 shows the reasons why the subject hospitals receive or do not receive dyslipidemia-related education fees. Of the subject hospitals, 66.7% do not receive the dyslipidemiarelated education fee and 48 hospitals of them responded that it was because of 'difficulty of making an education team.'
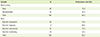
Table 3 shows the current status of dyslipidemia nutrition education. To the multiple-response question related to the types of dyslipidemia nutrition education, 13.0% responded 'group education', 82.0% 'individual education', 1.0% 'practice', and 4.0% 'group + individual education', and the average education fees were 6,500 KRW for group education, 14,498 KRW for individual education, and 32,625 KRW for group + individual education.
Job standards for clinical nutrition treatment of dyslipidemia
Definition of clinical dietitians for dyslipidemia was made first by the DACUM workshop. And then, after several meetings, clinical dietitians for dyslipidemia were defined as a professional who performs clinical nutrition treatment including self-management education and training to treat dyslipidemia and prevent complications of dyslipidemia for individuals and groups.
The job of clinical dietitians for dyslipidemia patients was analyzed based on the DACUM method, and the job specification included duties, tasks, and task elements. It was composed of 18 tasks and 53 task elements, which were organized in a table (DACUM chart) by duties (Figure 1). Here, the main duties of clinical dietitians were based on core duties defined in previous research [26], and, were in accord with the NCP steps of international confederation of dietetic associations (ICDA), 'A. nutrition assessment', 'B. nutritional diagnosis', 'C. nutrition intervention', and 'D. nutrition monitoring and evaluation.' The duties included specific tasks: for 'A. nutrition assessment,' A1. review basic information, A2. review medical history and treatment plan, A3. evaluate anthropometric data, A4. review laboratory and medical test, A5. review nutrition focused physical findings, A6. collect and evaluate data related to food and nutrition, A7. decide nutritional needs, and A8. document nutrition assessment; for 'B. nutritional diagnosis,' B1. derivate nutritional diagnosis, and B2. document nutritional diagnosis. 'C. nutrition intervention' C1. plan nutrition intervention, C2. management of nutritional prescription, C3. implement of nutrition intervention, C4. document nutrition intervention, and 'D. nutrition monitoring and evaluation,' D1. monitor nutritional status, D2. monitor the nutrition intervention process, D3. evaluate nutrition intervention, and D4. document nutrition monitoring and evaluation.
Based on these job descriptions, a specific job description was added to each task element and the tasks were classified as 'basic' and 'recommended.' 'Basic' means basic tasks that clinical dietitians must perform, whereas 'recommended' means tasks performed by experienced professional dietitians for dyslipidemia.
Field application evaluation
General information on the subjects and nutrition practice in medical institutions
Field application evaluation was performed by working clinical dietitians at 10 medium and large hospitals, and Table 4 shows general information on patients with dyslipidemia to whom the study was applied. Of the 30 patients, 17 were female and 13 male, and the average age was 54.2. Also, 14 were inpatients and 16 outpatients, and 21 received nutrition management only in the beginning while 9 received follow-up management as well. And, the average time for clinical dietitians to provide nutrition management for these patients was 43.8 minutes.
Job performance rate and difficulty
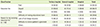
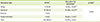
When the job standards were applied to the hospitals, of the 65 basic tasks, 76.9% was performed and, of the 35 recommended services, 52.5% was performed. Also, in terms of duties, 74.4% of the 52 nutrition assessment tasks, 86.0% of the 9 nutritional diagnosis tasks, 75.5% of the 23 nutrition intervention tasks, and 28.2% of the 16 nutrition monitoring and evaluation tasks were performed (Table 5). Table 6 presents the result of studying job performance by duty according to types of dyslipidemia patients. The performance rates of nutrition assessment, nutritional diagnosis, nutrition intervention, and nutrition monitoring and evaluation for inpatients were 67.1%, 69.7%, 76.7%, and 39.2%, respectively, and, for outpatients, 79.4%, 97.2%, 74.7%, and 20.7%.
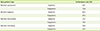
Table 7 presents the rate of coincidence for task difficulty between the researchers and clinical dietitians. The rates of coincidence for basic tasks, nutrition assessment, nutritional diagnosis, nutrition intervention, and nutrition monitoring and evaluation, were 85.6%, 62.5%, 56.8%, and 63.0%, respectively, while those of recommended services were 46.0%, 66.7%, 55.6%, and 54.0%.
Final version of job standards of clinical nutrition service for dyslipidemia
The draft job standards were shown to relevant institutions for advice and review, and, after field application evaluation and discussions, experts mainly suggested that the criteria for 'basic' and 'recommended' tasks need to be more specified; there are too many task elements and items in job description evaluation; and job standards for other diseases were needed as well. Also, the job standards and form developed based on field application evaluation were reviewed by institutions and all respondents were satisfied with the modified job standards. Later, based on field application evaluation and expert advice, the job standards were modified and supplemented, and the final job standards for clinical nutrition treatment of patients with dyslipidemia included 73 basic services and 26 recommended services, among 4 duties, 18 tasks, 53 task elements, and 99 job descriptions (Table 8).
Discussion
For the purpose of qualitative improvement of clinical nutrition service, in this study, the current status and practice of clinical nutrition service for dyslipidemia in Korean hospitals was studied, and job standards of clinical dietitians for clinical nutrition treatment of patients with dyslipidemia that can be applied to medical institutions were developed based on DACUM analysis and field application evaluation.
For dyslipidemia patients, it has been reported that improving diet through nutrition education and consultation can reduce risk factors and frequency of medication, and improve nutritional knowledge [27]. Therefore, clinical nutrition service provided by clinical dietitians has been reported to maximize treatment efficacy and reduce medical costs [15,28]. Also, clinical nutrition service for prevention and treatment of dyslipidemia is likely to become more important in the future as the prevalence of the disease grows every year. However, unlike in the U.S. where clinical nutrition service is applicable for health insurance benefits since 2002 [29], South Korea does not have no legislative policy relating to clinical dietitians and, therefore, does not insure the service. According to the result of this study, when patients receive nutrition education, individual education costs 24,487 KRW and group education 39,000 KRW. Therefore, if patients can receive insured clinical nutrition service, it may reduce prevalence and death rate of the disease.
Recently, it has been emphasized the tasks of clinical dietitians should be more specific and clear in order to activate services. A series of job activity analyses has been conducted for dietitians at schools, business places, hospitals, and health centers between 2002 and 2008 [23,24,25,30] and, in 2013, job standards of clinical dietitians at hospitals was developed [26] in Korea. This study was conducted based on previous research that suggested a wide range of tasks of clinical dietitians for overall diseases, and analyzed tasks that must be performed by clinical dietitians for clinical nutrition service of dyslipidemia. Here, to determine the tasks in a short period, the DACUM method was used, and the tasks and task elements were proposed according to the four steps of NCP, developed by AND (Academy of nutrition & dietetics, USA). This study may provide a manual for high quality clinical nutrition service by clinical dietitians performing standardized tasks, and to highlight the importance of clinical dietitians at hospitals who are in charge with diet and health management for patients.
The job standards for clinical nutrition treatment of patients with dyslipidemia proposed in this study include 4 duties, 18 tasks, 53 task elements, and 99 job descriptions, with less duties, tasks, and task elements than in the job description of clinical dietitians at hospitals developed by Cha et al. [26], which included 7 duties, 27 tasks, and 93 task elements. The tasks were reduced perhaps because the study was focused on tasks of clinical dietitians for a specific disease rather than overall diseases. Also, AND introduced job standardization for nutritional management since the early 2000s, and has published standard of practice (SOP) and standard of professional performance (SOPP) for clinical dietitians for various diseases [19,20]. While Cha et al. [26] proposed seven duties including nutrition assessment, nutritional diagnosis, nutrition intervention, nutrition monitoring and evaluation, consultation and cooperation, nutrition research, and self-development, this study, based on Korean and overseas studies, proposed four steps according to NCP; nutrition assessment, nutritional diagnosis, nutrition intervention, and nutrition monitoring and evaluation.
When the proposed job standards were applied to hospitals, the performance rate was high, average 68.3%, while the performance rate of nutrition monitoring and evaluation was the lowest, 28.2%. This low performance rate of nutrition monitoring and evaluation, despite the high importance can be explained by a lack of workforce and concentration on evaluation and management of patients. It is believed that inefficient communication with the medical staff in overall hospitals can induce difficulties in clinical nutrition services [31].
Therefore, in this study, job standards for clinical dietitians for dyslipidemia patients at hospitals were developed based on tasks that are most necessary. However, authors believe that there are limitations in applying the proposed job standards to different regions with different medical staff and practices. However, if such limitations are improved and job standards of clinical dietitians are continuously developed, the recognition and status of clinical dietitians will be improved within the hospital and the nation.
Conclusions
The definition and job standards of clinical dietitians for dyslipidemia were made based on DACUM analysis. The job standards included 4 duties, according to the steps defined in NCP, 18 tasks, 53 task elements, and 99 job descriptions, with 73 basic services and 26 recommended services. The job standards for clinical nutrition treatment for patients with dyslipidemia developed in this study can be effectively used in clinical fields and also improve quality of clinical nutrition service and quality of life of patients with dyslipidemia.




 XML Download
XML Download