

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The prevalence of atrial fibrillation is predicted to increase significantly as the elderly population increases [1]. Approximately 4% of Koreans aged over 80 years have atrial fibrillation [2]. Warfarin is a vitamin K antagonist that is prescribed for patients who are at increased risk of blood clot formation. Long-term anticoagulant therapy is required for patients with mechanical heart valves, chronic atrial fibrillation, and venous thromboembolism [3].
Warfarin produces an anticoagulant effect by interfering with the regeneration of vitamin K hydroquinone from vitamin K epoxide. It inhibits the reductase enzymes in the vitamin K cycle [4]. The international normalized ratio (INR) is used to monitor the effectiveness of the anticoagulants. If anticoagulant effect of warfarin is excessive, INR can be increased and bleeding can occur as a side effect. Reversely, if anticoagulant effect wears off, INR can be decreased and risk of blood clot increases [5]. Warfarin therapy requires close monitoring owing to its narrow therapeutic range [6]. Several factors such as age, alcohol consumption, diet, exercise, concomitant medications, and environmental changes are known to affect the response to anticoagulants [378]. Dietary vitamin K is an independent factor that influences changes in INR [9].
Vitamin K is a fat-soluble vitamin. Dark green vegetables, herbs, and vegetable oils are the major sources of the vitamin K [10]. Vitamin K provides function for blood coagulation by helping carboxylation of vitamin K-dependent coagulation factors. A high intake of vitamin K results in reduction of INR and low dose of vitamin K increases INR [9].
For a long time, many studies have been conducted on warfarin use for its drug and food interaction. A high intake of vitamin K is believed to be an inhibiting factor for anticoagulation therapy [11]. On the other hand, low intake of vitamin K has been recognized as a risk factor that causes instability of the anticoagulant effect. It has been addressed that it is required to reconsider restriction of vitamin K intake, as even a small change in diet by patients who restrict to vitamin K intake might cause fluctuation of the anticoagulant effect [12]. Lower variability of intake was found among individuals with high vitamin K intake and that might lead to have more stable anticoagulant therapy [13]. When patients receiving warfarin therapy were divided into stable INR group and unstable INR group, the mean daily intake of vitamin K in the unstable INR group was significantly lower than that in the stable INR group [14]. A study on the relationship of vitamin K intake and stability of anticoagulation control in patients taking long term warfarin confirmed that increasing vitamin K intake resulted in the reduction of warfarin sensitivity [15].
A goal of nutrition educations for patients receiving warfarin therapy is to minimize variance of vitamin K intake [161718]. Dietitians recommend that patients taking warfarin should maintain their vitamin K intake constantly and they instruct patients to be cautious for having a sudden vitamin K-rich food item [19]. Although the typical Korean diet includes vegetables high in vitamin K, assessment of vitamin K intake among Korean patients receiving warfarin therapy has not been adequately studied. This study aimed to explore the correlation between routine vitamin K intake and response to anticoagulant therapy among Korean patients receiving warfarin.
Materials and Methods
Subjects and study period
A retrospective survey of newly hospitalized Korean patients on continuous warfarin therapy was conducted. A total of 50 patients (aged between 21 and 87 years) were included in the study. Patients with short term warfarin therapy, patients newly prescribed warfarin therapy and patients taking additional anticoagulation (aspirin, heparin and etc.) with warfarin were excluded. This study was performed with the approval of the institutional review board of Seoul Saint Mary's Catholic Medical Center (KC15RISI0603). Informed consent was waived by the institutional review board because we retrospectively evaluated the previously acquired data.
Data collection
For each patient, clinical information and laboratory parameters including age, gender, body mass index (BMI), disease diagnosis, warfarin dosage, concomitant medications, INR results and duration of warfarin therapy were collected by reviewing the medical records. Alcohol, tobacco, dietary supplement use and past history of dietary vitamin K intervention during warfarin therapy were determined by medical records and interview.
Assessment of anticoagulation effects
Anticoagulation effect was evaluated by using the percent time in therapeutic INR range (TTR). TTR is a validated indicator of anticoagulation effect. It has been used to determine how long the patient might have been within their therapeutic range. TTR was calculated with the method designed by Rosendaal et al. [20]. Briefly, Rosendaal TTR is assessed by using linear interpolation between consecutive INR values. The therapeutic INR range was 2.0 to 3.0 for most patients and 2.5 to 3.5 for patients with artificial valve replacement. To evaluate stability of anticoagulant effect, we used the coefficient of variation (CV) of INR [15].
Assessment of usual vitamin K intake
We estimated usual vitamin K intake based on a semi-quantitative food frequency questionnaire (FFQ) that has been designed for the purpose of assessing dietary intake of vitamin K [21]. Thirty four items were included by selection of major phylloquinone resources based on the data in the Fifth Korea National Health and Nutrition Examination Survey [22]. Main food sources for vitamin K intake of Koreans, such as cabbage kimchi, spinach, laver, soybean oil, fermented soybean and etc. were included. Response options for food frequency toward each item were never or less than once per month, once per month, 2-3 times per month, 1-2 times per week, 3-4 times per week, 5-6 times per week, daily, 2 times per day, 3 times per day. Standard portion size were specified for each item in amount choices of small (50%), medium (100%) and large (150%). The FFQ records were obtained through face to face interviews by a registered dietitian.
Statistical analysis
Statistical analyses were performed using SAS software (version 9.4, SAS Institute, Cary, NC, USA). Usual vitamin K intake was calculated using CAN-Pro (version 4.0, The Korean Nutrition Society, Seoul, Korea). General characteristics and disease related characteristics were expressed in mean ± standard deviation and percentage. Study subjects were divided into tertiles according to their usual vitamin K intake. General and clinical characteristics of patients were compared among the three groups by the one-way analysis of variance (ANOVA) and the Chi-square tests. Wilcoxon rank-sum test and Kruskal-Wallis test were used to compare usual vitamin K intakes across subgroups. The anticoagulant effect is influenced by confounding factors, including demographic data, alcohol consumption, smoking and diet [3723]. Correlations (both crudely and after adjustment for potential confounding factors) between usual vitamin K intake and anticoagulant effects were assessed by Spearman rank correlation coefficient test. Statistical significance was set at a value of p < 0.05.
Results
General and disease-related characteristics
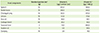
General and clinical information for the study subjects were represented in Table 1. Mean age of the patients was 66 years old, and 64.0% of study subjects were older than 65 years old. Study subjects were divided into tertiles according to their usual vitamin K intake. Usual vitamin K intake was 45.2-150.8 µg/day for the first tertile, 164.5-326.9 µg/day for the second tertile and 328.9-757.9 µg/day for the third tertile. The proportion of men was significantly higher in second and third tertile than first tertile (p = 0.028). The proportion of subjects who currently use of dietary supplement, alcohol and tobacco were 32.0%, 18.0% and 8.0%. The clinical indications for warfarin therapy were atrial fibrillation (46.0%), valve replacement (26.0%), thrombosis and other disease (28.0%). The mean duration of warfarin therapy was 48.8 months and 56.0% of study subjects received warfarin therapy over 3 years. The mean daily dose of warfarin was 3.2 mg (1.0 to 7.5 mg) and mean number of concomitant drugs was 5.4.
Vitamin K intake
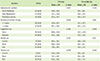
The mean vitamin K intake was 262.8 ± 165.2 µg/day. There was high inter-individual variation of usual intake of vitamin K (45.2-757.9 µg/day). The average usual intake of vitamin K was higher in men compared with women (289.0 ± 166.6 µg/day for male and 216.2 ± 156.3 µg/day for female). Main food components to dietary vitamin K1 intake of subjects were represented in Table 2 [22].
Anticoagulant effect
Percent TTR and CV of INR were used to evaluate anticoagulant effect in the study. Table 3 shows anticoagulant effects within subgroups. The mean percent TTR was 38.4 ± 28.4% and the range of TTR was 5.8 to 91.7%. Long-term warfarin therapy group (≥ 3 years) had higher percent TTR than control group (< 3 years) (p = 0.046). The mean CV of INR was 31.8 ± 11.8%.
Relationship between usual vitamin K intake and anticoagulant effect
The relation of usual vitamin K intake and anticoagulant effect was represented in Table 4. No statistically significant correlation was found between usual vitamin K intake and percent TTR. The same results were found after adjusting for confounding factors, such as age, gender, BMI, use of alcohol, tobacco and dietary supplements.
Discussion
Warfarin is a medication for preventing blood clot and diseases such as stroke and myocardial infarction caused by blood clot. However, anticoagulation effect of warfarin is affected by environmental changes of patients including dietary vitamin K [7]. Fluctuation of anticoagulation effect results in INR to be out of therapeutic range and thrombosis, bleeding events and mortality increase [24]. Therefore, it is important to minimize the fluctuation of anticoagulant effects and manage INR to be stabilized within the therapeutic range.
Few studies have been reported relationship between dietary vitamin K and anticoagulant effect. It has been reported that higher vitamin K intake is significantly associated with higher percent TTR [25]. A study on the correlation between Mediterranean diet and quality of anticoagulation confirmed that Mediterranean diet is not associated with changes in TTR [26].
Many of the patients in this study have expressed difficulties in diet control. It is observed that some of the subjects tried to completely restrict foods high in vitamin K. Anticoagulated patients are often advised to avoid foods high in vitamin K [27]. Dietary intervention that limits the intake of foods high in vitamin K may lead to excessive restriction of vitamin K intake in patients receiving warfarin therapy. When restricting vitamin K intake excessively, fluctuation of vitamin K intake can be increased and cause instability of INR [2829]. European Society of Cardiology recommended that dietary recommendations for warfarin treated patients should not be aimed at avoiding vitamin K-rich food items, but at trying to maintain a stable and not-too-low daily intake [30].
Only limited numbers of studies have been performed for nutrition intervention strategy which can be tried for patients receiving warfarin therapy. A strategy to adjust a frequency of intake of the food high in vitamin K was suggested [31]. This strategy could help to maintain INR within the therapeutic range. However, adherence of patient can be decreased as it is inconvenient to adjust the meal strategy whenever INR fluctuate. Another strategy to maintain weekly vitamin K scores was designed [32]. Vitamin K-rich vegetables were classified into seven score grades according to their relative vitamin K content per serving. This strategy seems to be applicable for the Korean patients.
In this study we could not find statistically relevant correlation between usual vitamin K intake of the patients taking warfarin and TTR, and CV of INR. The possible causes of the results can be inferred by the followings. First of all, there was a possibility that the accuracy of the vitamin K intake assessment has been lowered. In this study, we included phylloquinone (vitamin K1) intakes only, in assessment of usual vitamin K intake and menaquinone (vitamin K2) intake was not assessed due to the lack of data. Also, as some of menaquinone which are synthesized by bacterial flora are absorbed in body [33], dietary intake may underestimate the intake. Lastly, there could be intra-individual differences in bioavailability of dietary vitamin K [27]. Therefore, further studies are required to consider the plasma vitamin K level in addition to vitamin K intake.
The strength of the study is that this is the first study performed to determine the correlation of TTR and usual vitamin K intake by investigating Korean anticoagulated patients. We reflected usual vitamin K intake by performing FFQ for the recent one year. The FFQ are consisted of high contributing items to vitamin K intake and reflect eating habits of the Korean [22].
This study has several limitations. The study is performed only for the patients taking warfarin who are hospitalized in a university hospital located in Seoul. Secondly, we need further validation on FFQ used to figure out usual vitamin K intake of subjects. Validity check was not fully performed in sufficient level for FFQ in this study, however, strong correlations were observed (r = 0.852) between FFQ and 5-days dietary record [21].
Conclusion
No significant association was observed between usual vitamin K intake and anticoagulant effects. Further studies are required to consider inter-individual variability of vitamin K intake. Development of assessment tools to measure inter-individual variability of vitamin K intake might be helpful.


 XML Download
XML Download