

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Metabolic syndrome (MetS) is a clustering of metabolic disorders such as abdominal obesity, dyslipidemia, elevated blood pressure, and high levels of blood glucose [1]. According to the world reports, the age-adjusted MetS prevalence has been estimated 34.2% between 1999 and 2006 in the US [2] and 31.3% in 2007 in Korea [3]. Although MetS accelerates the risk of developing chronic diseases such as atherosclerosis, cardiovascular disease, and diabetes [4], the exact pathologic mechanisms of MetS have not been identified.
Previous studies, across the observational [567], prospective [89], and meta-analysis study designs [10], have speculated that type of dietary fat and plasma fatty acid (FA) composition contribute to development of insulin resistance and MetS. Furthermore, the intervention studies reported that a change of fat composition in diet affects on a composition of plasma FA as well as metabolic dysfunction [1112]. While polyunsaturated FA (PUFA) intake has been reported by its inverse association with the risk of metabolic dysfunction [1314], the intake of saturated FA (SFA) has been associated with its adverse effects on the risk of MetS [1516]. It is a well established fact that palmitic acid (16:0) and stearic acid (18:0) have atherogenic and cardiovascular effects [1718]. However, recent studies have suggested that each SFAs have different effects on metabolic conditions according to their chain length [19]. SFAs with 20 or more carbon atoms such as arachidic acid (20:0), behenic acid (22:0), and lignoceric acid (24:0), were classified as very long chain SFAs (VLSFAs). Previous studies on that VLSFAs reported that intakes of VLSFA have beneficial effects on the metabolic abnormalities, including diabetes and cardiovascular diseases [1202122]. However, the association between dietary VLSFAs and MetS has not been fully understood.
With respect to nutrition transition the intake of saturated fat has been considerably increased in the Korea. Therefore, we aimed to evaluate the effect of VLSFAs intake on metabolic parameters. Additionally, we also examined the association between dietary VLSFAs intake and MetS prevalence in Korean population.
Materials and Methods
Study population
This study was based on data from the Korea National Health and Nutrition Examination Survey (KNHANES) VI (2013), the cross-sectional survey conducted by a Ministry of Health and Welfare. Details of the KNHANES are available elsewhere [23]. The KNHANES is composed of the three sections such as a health interview, health examination, and nutrition survey. A nationally representative sample was chosen from the Korean population using household records that were provided by the 2010 Population and Housing Census in Korea. In the KNHANES VI, 8,018 participants was selected from each 192 survey section using a stratified, multistage probability cluster sampling method considering each participant's geographical area, age, and sex (response rate: 79.3% for age ≥1 year). Among the participants, we limited our analyses to adults who is older than 20 years old. We also excluded subjects with missing data for important analytic variables, such as metabolic parameters, and FA intake. Subjects who recorded implausible energy intake (<500 kcal or >5,000 kcal) were excluded. Additionally, subjects who were diagnosed with severe disease such as cancer were excluded. Pregnant or lactating female subjects were excluded due to their unique changes in hormonal status. Finally, 4,232 subjects were included in the statistical analysis. The institutional review board of the Centers for Disease Control and Prevention in Korea approved the KNHANES. All participants in the survey provided informed consent form.
General characteristics of the subjects
We obtained data from KNHANES VI, including demographic, anthropometric, and biochemical measurement data. Demographic variables that were potential confounders including age, education, alcohol use, smoking status, physical activity, nutrient supplementation use, and disease status. Subjects who smoked during the survey period were regarded as current smokers. Subjects who consumed alcohol at least once a month considered as current alcohol consumers. Education level was divided into four categories as elementary school, middle school, high school, or university, according to the subject's highest achieved level. Physical activity was divided into two categories, exercise or do not exercise as an activity of the following at least 5 days a week: intense physical activity for at least 20 minutes, moderate physical activity for at least 30 minutes, or walking for at least 30 minutes. Nutritional supplement use was divided into two categories as "yes" or "no".
Anthropometric and biochemical measurements
Anthropometric measurements were obtained by trained experts following standardized protocols. The body weights and heights of the subjects were measured to the nearest 0.1 kg and 0.1 cm, respectively. Body mass index (BMI) was calculated as weight (kg)/height squared (m2). Waist circumference (WC) was measured on the area between the rib cage and the iliac crest to the nearest 0.1 cm. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured by mercury sphyngmomanometer (Baumanometer, New York, NY, USA) on the right arm. To assess serum levels of biochemical markers, blood samples were collected through an antecubital vein after 10-12 hour of fasting. Serum levels of insulin (µU/mL) were measured by an immunoradiometric assay using a 1,470 Wizard Gamma Counter (PerkinElmer, Turku, Finland). Hemoglobin A1c (HbA1c) level was measured with high performance liquid chromatography-723G7 (Tosoh, Tokyo, Japan). Serum levels of fasting glucose (mg/dL), total cholesterol (TC, mg/dL), triglyceride (TG, mg/dL), high density lipoprotein (HDL) cholesterol (mg/dL), low density lipoprotein (LDL) cholesterol, aspartate aminotransferase (AST, IU/L), and alanine aminotransferase (ALT, IU/L) were measured using a Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan). To compensate the missing data, LDL cholesterol was calculated by Friedewald formula for subjects in less than 400 mg/dL TG: TC (mg/dL) - HDL cholesterol (mg/dL) - (TG (mg/dL) ÷ 5.0) [24].
Dietary fatty acid measurement
Nutrient intake data were obtained from the section of the nutrition survey in the KNHANES (VI). Food content and consumed amounts were obtained by the 24-hour recall method; then, the nutrient intake was analyzed using the database from the food composition table made by the Rural Development Administration [25]. The ratio of energy intake from each macronutrient to total energy was calculated: percentage of energy intake from carbohydrate (%), percentage of energy intake from fat (%) and percentage of energy intake from protein (%). The percentages of energy intake from VLSFAs (%) were also calculated as same method.
Definition of metabolic syndrome and other disease
According to National Cholesterol Education Program criteria [26], MetS is defined by a co-occurrence of three or more of the following conditions: 1) waist circumference >90 cm in men >80 cm in women using the International Obesity Task Force criteria for the Asian-Pacific population [27]; 2) TG ≥150 mg/dL or medication use; 3) HDL-cholesterol <40 mg/dL in men and <50 mg/dL in women or medication use; 4) blood pressure ≥130/85 mmHg or anti-hypertensive medication use; and 5) fating glucose ≥100 mg/dL or medication use (insulin or oral agents). Disease status was defined using self-reported questionnaires and examination. Subjects were defined as having hypertension (HTN) if they were diagnosed with hypertension by physician, had high blood pressure (≥140/90 mmHg), or took anti-hypertensive medication. Diabetes was defined as subjects who were diagnosed with diabetes, had high levels of fasting blood glucose (≥126 mg/dL), or used anti-diabetic medication. Subjects were defined as having hyperlipidemia if they were diagnosed with hyperlipidemia, had high levels of TC (≥240 mg/dL), or took medication. Cardiovascular disease (CVD) included HTN, stroke, myocardial infarction, and angina pectoris.
Statistical analysis
Statistical analyses were performed using Stata SE 12.0 (Stata Corp, College Station, TX, USA). Continuous variables were described as means ± standard error, and categorical variables were expressed as percentage of subjects. We compared demographic factors and clinical measurements according to quartiles of VLSFA intake, using one-way ANOVA with Bonferroni's correction for multiple comparisons. Chi-square test was used to determine statistical difference in categorical variables. Logistic regression was used to obtain estimates of the VLSFA intake for MetS with the two described models. The first model was adjusted for age and sex. The second model was adjusted for age, sex, BMI, education level, alcohol use, smoking, exercise, coexistence of CVD, and intake of nutrient supplement. For the regression analyses, levels of FA were divided into quartiles. All analyses were performed after testing of normal distribution. For all analyses, p-values < 0.05 were considered significant.
Results
General characteristics of subjects
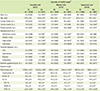
Median level of arachidic acid intake in the diet was 0.04% (0.00%, 0.42%). Median level of behenic and lignoceric acid intake in the diet were 0.01% (0.00%, 0.66%), and 0.001 (0.000%, 0.363%), respectively. The general characteristics of subjects are presented in Table 1. The mean age of the total study population was 49.7 ± 0.2 years (range: 20-92 years), and 42.3% of the total subjects were men. Subjects with higher levels of arachidic and behenic acid were younger, more exercised, achieved higher levels of education, and had lower prevalence of CVD, HTN, diabetes, and dyslipidemia compared to their lowest quartile group (all p < 0.05). Subjects with higher levels arachidic and lignoceric acid had lower proportion of current smoker and alcohol user. Highest quartile groups of behenic and lignoceric acid intake used more nutrient supplementation (p < 0.05). Nutrient intake of subject across the quartiles of VLSFAs are also presented in Table 1. Subjects with higher levels of any of the three kinds of VLSFAs showed higher intake of protein and fat (p < 0.05). Especially, they consumed higher levels of mono-unsaturated FA (MUFA) and PUFA compared with those with lower levels of these three VLSFAs (p < 0.05).
Biochemical measurement according to intake of VLSFAs
To evaluate the effect of VLSFAs intake, we compared the levels of metabolic risk factors across the quartiles of each VLSFAs intake (Table 2). Subjects with higher levels of any of the three VLSFAs showed favorable metabolic status, including lower levels of circulating TG (p < 0.05). Subjects in highest quartile group of arachidic acid and behenic acid intake showed lower levels of BMI, WC, blood pressure, blood glucose, and AST (all p < 0.05), and higher level of HDL cholesterol (p = 0.0003) compared to their lower quartile groups.
Association of intake of VLSFA and prevalence of metabolic syndrome
Based on differences in metabolic risk factors, we further examined the cross-sectional associations of VLSFAs with prevalence of metabolic syndrome (Table 3). Higher intakes of arachidic acid was negatively associated with MetS before and after adjustment (odds ratio [OR]: 0.66, 95% CIs: 0.51, 0.85). Also, after adjustment for potential confounders, sum of intake levels of VLSFAs was associated with lower risk of MetS (OR: 0.75, 95% CIs: 0.59, 0.96). However, there is no significant association between intakes of behenic or lignoceric acid and MetS, in individual manners.
Discussion
In the present study, we observed significant differences in metabolic risk factors such as WC, blood pressure, and lipid traits according to levels of dietary VLSFAs intake among the Korean population. In the cross-sectional design, subjects with higher intake of the arachidic acid indicated significantly lower prevalence of MetS. Moreover, total intake of arachidic acid, behenic acid, and lignoceric acid showed a protective effect against the risk of MetS.
Arachidic acid, behenic acid, and ligonoceric acid are contained in peanuts, canola oil, cashew nut and macadamia nuts [28]. Although we could not utilize plasma levels of VLSFAs, dietary VLSFAs consumption are generally known to influence plasma levels of VLSFAs [29]. In dietary intervention studies, intakes of macadamia nut, which contains plenty of VLSFAs, elevated plasma levels of VLSFAs and lowered plasma TC and LDL-cholesterol level [3031]. VLSFAs attached in phospholipids are synthesized endogenously by elongation of palmitic acid (16:0) and stearic acid (18:0). Elongases such as elovl1, elovl3, and elovl7 are involved in elongation process in the endoplasmic reticulum [32]. Generally, palmitic and stearic acid, which are derived from animal products, have been reported to have adverse effects on CVD, and inflammatory responses [15161718]. However, the metabolic factors which regulate the conversion of stearic fatty acid into VLSFAs have been unknown [20].
Although the biological mechanism underlying chain length and its distinct effects are not clear, our finding supports diverse metabolic effect of VLSFAs. Beneficial effects of VLSFAs in our results are consistent with previous findings [20212232]. Large population-based studies reported that the protective effects of VLSFAs on atrial fibrillation and sudden cardiac arrest [2132]. Additionally, Fretts et al. [21] reported that a group of subjects in highest level of plasma VLSFA showed 22% (20:0), 38% (22:0), and 32% (24:0) lower risk of atrial fibrillation (AF) respectively. They speculated that VLSFA may prevent apoptosis, which is a main pathophysiology of AF, including fibrosis and the progressive atrial remodeling leading to vascular diseases [33]. Unfortunately, distinct functions of VLSFA are still controversy. Matsumori et al. [1] reported that the level of arachidic acid in erythrocytes was correlated with atherogenic lipid traits in subjects with MetS. Also, one case-cohort study reported that higher quintile of erythrocyte membrane contents of behenic and lignoceric acid were associated with increased risk for type 2 diabetes [34].
Since different VLSFAs have distinct biological functions compared to other SFAs, their association with cardiometabolic risk factors such as insulin resistance are varied [35]. VLSFAs, major elements of ceramides and sphingomyelins affect liver homeostasis, myelin maintenance, and anti-inflammatory response through ceramide synthase expression [36]. Mesicek et al. reported that ceramides properties depended on the chain length of fatty acid, and ceramides produced by lignoceric acid (24:0) and nervonic acid (24:1) exerted protective effects on insulin resistance induced apoptosis in HeLa cells [37]. In other experimental studies, decreased expression of ceramide synthase in mice increased susceptibility to insulin resistance through decreased levels of VLSFA-derived sphingolipids [3839]. Furthermore, ceramide synthase 2-deleted mice showed increased level of palmitic acid-derived ceramides in their liver to compensate depleted levels of C22-24 ceramides, and developed hepatopathy [40]. Taken together, the VLSFAs may contribute to lower risk of MetS through endogenous ceramide synthesis. The biological mechanism underlying the association between MetS and VLSFAs needs to be specified with further study.
There are several limitations in the present study. First, a causal relationship between dietary intake of VLSFAs and MetS cannot be estimated since this is a cross-sectional study. Second, the study population size was small without a healthy control group who did not have any metabolic risk factors. Finally, dietary intake of VLSFAs were based on 24-hour recall method, which can be biased by recent SFA intake. Moreover, we could not consider the absorption rate of VLSFAs within the human body since we do not have information of food source and plasma levels of the VLSFAs. Despite of these limitations, the present study has strengths above other studies. This is the first study to investigate the association between dietary VLSFAs and MetS in Korean population. We compared whether each VLSFAs were associated with MetS using a nation-wide scale survey data of homogeneous subjects. Furthermore, coexistence of CVD and nutrient supplementation were adjusted to minimize potential confounding factors.
Conclusion
Our results corroborate that intake of VLSFAs may have beneficial effects on metabolic risk factors in Korean. Specifically, intake of arachidic acid was significantly associated with lower risk of MetS. Considering the prevalence of MetS in Korea, the present study may contribute to preventing and decreasing risk for MetS among Korean population. Further interventional study is necessary to understand the causal effects of dietary intake of VLSFAs and their endogenous metabolism related to the risk of MetS.


 XML Download
XML Download