

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Nephrolithiasis, or kidney stone, is the presence of renal calculi caused by a disruption in the balance between solubility and precipitation of salts in the urinary tract and in the kidneys. The incidence is at peak among white males age 20 and 30 years old. The National Health and Nutrition Examination Survey (NHANES) III (1988-1994) reported that there was a 5% prevalence of stone formation among adults in the United States and this represented a 4% increase from the NHANES II (1976-1980) [12]. Nephrolithiasis is considered to be a disease of affluence like obesity, hypertension, and type 2 diabetes because it is so prevalent in wealthy countries [34]. Urologic intervention is required in as many as 20% of patients with renal colic [5] and more than $2 billion is spent on treatment each year. The lifetime prevalence of kidney stones in the United States is 12% among men and 7% among women [67]. Kidney stones develop when urine becomes "supersaturated" with insoluble compounds containing calcium, oxalate (CaOx), and phosphate (CaP), resulting from dehydration or a genetic predisposition to over-excrete these ions in the urine. About 5-10% of Americans have this predisposition.
Kidney stone formation
When CaOx concentration is 4 times above the normal solubility a crystal starts to form. If the CaOx concentration is 7 to 11 times higher than normal solubility the nucleation begins. In low urine volume, the presence of high calcium, high oxalate the supersaturation (SS) of CaOx is increased. Citrate in the urine forms soluble complex with urinary Ca. If urine has low citrate concentration SSCaOx is promoted to form CaOx stone. If urine pH is > 6.5, proportion of divalent and trivalent ions are increased then SSCaP is favorable. The levels of urinary supersaturation of the different solutes determine the specific types of stones [8910].
Kidney stones tend to recur. Approximately 50% people who form one stone form another within 10 years. The risk of recurrence ranges from 30-50% at 5 years in observational studies. The control groups in recent randomized controlled trials have a 2-5% annual recurrence rate after an incident calcium oxalate stone. Recurrence rates also depend on the stone type. When nuclei of uric acid form, they lower the metastable limit (e.g. susceptibility to perturbation) and favor further stone precipitation. Decreased supersaturation of the urine filtrate will decrease the risk of recurrence of kidney stone [11].
Types of Kidney Stones
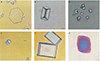
Table 1 describes the various types of kidney stones and their prevalence. Approximately 70-80% of kidney stones are composed of calcium oxalate and calcium phosphate. Of the rest, 10% are struvite, 10% of uric acid; and less than 1% are composed of cystine or are diagnosed as drug-related stones. Calcium and uric acid stones are more common in men; women have more struvite stones. Figure 1 shows the appearance of the different types of stones.
Calcium stones
Most calcium stones are composed of calcium oxalate, either by itself or much more commonly in combination with calcium phosphate or calcium urate [913]. Hypercalciuria, low urine volume and hypocitraturia all predispose to the development of calcium stones. Hypercalciuria often occurs with diseases associated with hypercalcemia like hyperparathyroidism, malignancy, sarcoidosis and vitamin D excess [1415]. When no other cause is found the hypercalcuria is known as "idiopathic hypercalciuria". Idiopathic hypercalciuria is familial and is likely a polygenic trait, although there are some rare monogenic causes of hypercalciuria and kidney stones such as Dent's disease, an X-linked disorder characterized by hypercalciuria, nephrocalcinosis, and the development of renal failure. Alkaline urine is a risk factor for the development calcium phosphate stones [111617]. Another risk factor for calcium oxalate stone is hyperoxaluria, which occurs due to bowel disease (enteric hyperoxaluria) and genetic disorders of oxalate metabolism (primary hyperoxaluria) [18].
Dietary oxalate may be important in stone development; spinach, beets and rhubarb in particular, contain large amounts of oxalate and they may increase urinary oxalate excretion and predispose to the development of calcium oxalate stones. High dose vitamin C therapy can also lead to increased oxalate generation as vitamin C (ascorbic acid) is metabolized. Oxalate reabsorption in the colon is reduced by the formation of insoluble calcium oxalate [192021222324].
This is very important in planning therapy because restricting dietary calcium results in less calcium being available in the intestinal lumen to bind the oxalate. This leads to increased oxalate absorption and therefore increased urinary oxalate excretion [21252627]. Therefore, dietary calcium should not be restricted in malabsorption syndromes such as small bowel disease, following surgical small bowel resection, jejuno-ileal bypass surgery and inflammatory bowel disease (IBD) in which there is malabsorption of fatty acids and bile salts. Intestinal calcium binds to fatty acids, causing less binding to oxalate. Non-absorbed bile salts in the colon will also cause increased colonic permeability to oxalate. Bariatric (weight loss) surgical techniques that create a malabsorptive state are being performed more frequently today than ever before. Calcium oxalate stone formation is an increasingly common complication with the more restrictive procedures, due to the highly restrictive forms of bariatric surgery such as the Roux-en-Y gastric bypass, sleeve gastrectomies and duodental switches with biliopancreatic diversion that generate malabsorption syndromes. Diarrheal losses cause volume depletion and decreased urine volume. Bicarbonate loss in the stool can cause a metabolic acidosis which can in turn lead to a low urinary pH and hypocitraturia (due to enhanced proximal reabsorption) which will predispose to the development uric acid and calcium oxalate stone formation [2829].
Uric acid stones
Pure uric acid calculi are radiolucent on plain radiographs but visible on ultrasonography or computerized tomography (CT). These stones tend to form in individuals with hyperuricosuria. Approximately 15-20% of patients with uric acid stones have a history of gout [30313233]. A diet rich in animal protein, because of its high purine content, which produces uric acid in its catabolism, may increase the risk of uric acid stone formation [323435]. At a urinary pH of less than 5.5, uric acid is poorly soluble, but solubility increases at a pH greater than 6.5.
Cystine stones
These stones tend to form only in patients with cystinuria, an autosomal recessive disorder affecting 1 in 15,000 adults in the USA that accounts for only 1% of patients with nephrolithiasis. In cystinuria, nephrolithiasis is the only clinical manifestation and it arises as a result of abnormal renal tubule transport which in turn leads to large amounts of urinary cystine excretion. Cystinuria occurs equally in males and females, although males are more severely affected. Stones begin to form in the 1st to 4th decades of life and tend to be large, multiple and bilateral. The diagnosis can be made by finding typical hexagonal crystals in the urine [3637]. Urinary tract infection and obstruction are common, as is stone recurrence every 1-4 years.
Struvite stones
Struvite stones are also called triple phosphate stones, or infection stones. They form in the presence of upper urinary tract infections with urease-producing bacteria (most commonly Proteus and Klebsiella). Normal urine is undersaturated with ammonium phosphate; struvite stone formation occurs only when ammonia production is increased and the urine pH is elevated, which decreases the solubility of phosphate. Bacterial urease is essential for the development of struvite stones because it leads to an elevation in ammonium, carbonate and urinary pH all at the same time. In this setting phosphate combines with ammonium, magnesium and carbonate to form a stone composed of magnesium ammonium phosphate (struvite) and calcium carbonate-apatite.
Resulting in increased availability of ammonium in an alkaline urine.
Struvite stones commonly occur in patients with recurrent urinary tract infections, especially if they have abnormal urinary tract anatomy, or require frequent bladder catheterization. The stones may also occur on infected calcium, uric acid or cystine stones, especially after instrumental procedures. Struvite stones are three times more common in women than men, presumably because urinary tract infections are more common in women. They are typically very large and may be so large as to fill the renal pelvis (forming a "Staghorn calculus"). Their growth is rapid and they often grow back after surgical removal because infected fragments of stone have been left behind [383940].
Clinical Diagnosis of Kidney Stones
Non-obstructing kidney stones produce no symptoms or signs apart from hematuria. However, the kidney stone may cause severe pain, usually accompanied by nausea, vomiting and hematuria (renal colic) when it passes into the ureter. Patients may also complain of urinary frequency and urgency. These signs and symptoms lead to many emergency department visits and hospitalization. The pattern of the pain from stone depends on its location: a stone in the upper ureter leads to pain in the flank that may radiate to the upper abdomen.
When the stone is in the lower ureter, pain may radiate to the ipsilateral testicle in men or labium in women. If the stone is lodged at the ureterovesical junction, the main symptoms will be urinary frequency or urgency. Symptoms quickly improve after passing the stone. On physical examination, the patient is often in excruciating pain, and is unable to achieve a comfortable position. Ipsilateral costovertebral angle tenderness may also be present.
Laboratory tests may show a leukocytosis which may be due to a stress response or infection. Serum creatinine is often elevated if the patient is volume depleted, or if there is bilateral ureteral obstruction or unilateral obstruction in a patient with a solitary kidney. The urinalysis will have red blood cells, white blood cells and occasionally crystals. However, because of the often non-specific physical examination and laboratory findings, imaging studies are critical in making the diagnosis.
Initial evaluation includes obtaining a non-contrast helical CT, which can accurately visualize the size and location of the stones. A kidney, ureter and bladder (KUB) film, although it is insensitive to uric acid stones since they are radiolucent and therefore are not visualized. However, it can visualize calcium - containing, struvite and cystine stones in the kidney or ureter. Complete ureteral obstruction and upper urinary tract infection (UTI) are indications for stone removal by extracorporeal shock wave lithotripsy (ESWL) or surgery [912163141].
Medical and nutrition evaluation of kidney stones
A comprehensive history should be taken by one of the health care providers, and the following items should be covered: prior kidney stones, composition of prior stones if known, dietary history including an estimate of typical daily fluid intake, social history including details regarding occupation and lifestyle, and family history.
The medical history should focus on identifying diseases that increase stone risk including conditions that lead to hypercalciuria, gout, chronic diarrhea and malabsorptive gastrointestinal disorders.
Interpretation of biochemical and urine tests
Urine
The urine sediment should be examined for crystals. A 24-hour urine collection should be performed to measure urine calcium, oxalate, uric acid, pH, volume, creatinine and citrate. Some laboratories calculate supersaturation values for calcium oxalate, calcium phosphate and uric acid and these are particularly helpful [124243].
The 24-hour urine collection
The best way to evaluate stone risk is a 24-hour urine collection and analysis [812]. Two 24-hour urine collections are recommended for the initial evaluation for an accurate analysis and to determine variability [44]. The 24-hour urine collection should be several weeks after any procedures (i.e. 6-8 weeks after lithotripsy) in order to minimize the risk of result be being influenced by infection or presence of blood due to these causes. Infection can change the pH and citrate levels. It is very important that patients continue with their usual diet and activities during the collection period. The 24-hour urine creatinine excretion can give information about the adequacy of the urine collection. In general, adult males produce 18-24 mg creatinine/kg/d and females 15-20 mg/kg/d [912]. 24-hour urine collection is not accurate as the urinary creatinine levels will be higher than normal for over collection and lower than normal for under-collection [44].
Table 2 provides a summary of the normal values for the 24-hour urine collection and likely causes of abnormal values. The 24-hour urine sample should include volume, and the solutes calcium, phosphorus, oxalate, citrate, pH, and uric acid to provide an estimate of supersaturation and the risk of stone formation. Creatinine is tested to ensure full collection and to normalize solute excretion to the more constant amount of creatinine. Dietary factors include sulfates which are mostly from animal protein and sodium since they are related to calcium, potassium, and magnesium excretion. Urea nitrogen is used to estimate protein catabolic rate (PCR). The PCR is usually indicative of dietary protein intake in an individual who is not in a catabolic state. The relationship between urinary nitrogen appearance rate and estimated dietary protein intake is then calculated. The value of the 24-hour urine is to evaluate dietary nutrients and fluid intakes and to provide guidance for the patient's management. For example, normal urinary calcium levels are <250 mg/d for men and <200 mg/d for women. High urinary calcium may be caused by idiopathic hypercalciuria, or diet high in sodium or protein. Low urinary calcium is often due to malabsorption or underlying bone disease. A normal urinary oxalate level is 20-40 mg/d. High levels are due to high oxalate diet, increased endogenous production, high vitamin C consumption and irritable bowel disease. Normal urinary citrate levels are >450 mg/d for men and >550 mg/d for women. High animal protein diets and renal tubular acidosis (RTA) can increase acid production affecting urinary pH so that it declines citrate levels.
Nutrition assessment
The dietitian's role in nephrolithiasis care is very important. The dietitian should assess nutritional risk factors by dietary intake assessments and provide therapeutic recommendations based on dietary risks. Dietary assessment is very important both in treating and preventing stone formation. The dietitian should evaluate dietary intakes of calcium, oxalates, sodium, protein (both animal and plant), dietary supplements and fluid intake since these can either promote or inhibit stone formation, and plan the therapeutic diet based on those information. Fluid intake is particularly important to quantify.
There are several dietary assessment methods: the 24-hour recall, food record diet history and food frequency questionnaire. The dietary intakes should be reflected on the urinalysis and it is good way to evaluate the causes of kidney stones and to prevent recurrence. Food records provide information on intake of foods, beverages, and dietary supplements over specific periods. The most appropriate diet assessment for kidney stones is the food record during a 24-hour urine collection, as well as 1-2 days before the collection. The food record should be analyzed to evaluate intakes of protein, sodium, potassium, calcium, phosphorus, magnesium, uric acid, oxalate and fluid. Based on the food intake and urinalysis, the clinicians can provide the adequate medical and diet treatments.
Risk Factors for Kidney Stones
Major risk factors
Risk factors for stone formation may be hereditary or disease related, such as idiopathic hypercalciuria, hyperoxalosis Dent's disease, medullary kidney disease, polycystic kidney disease, hyperparathyroidism, irritable bowel disease (IBD), renal tubular acidosis or sarcoidosis. Patients with a family history of nephrolithiasis have a 2.5 times greater risk of stone formation [42]. Other risk factors include environment and diet (Table 3).
Table 4 shows the conditions that favor stone formation. Urinary crystalloids can form nucleus on the existing surface and supersaturate urine. Low urinary magnesium causes decrease complex formation with urinary oxalate allowing free oxalate to be more available in the urine. Low urinary citrate also increases stone formation because citrate forms a complex with calcium so free calcium is more available for stone formation. High concentrations of uric acids in the urine will promote the nuclei to start stone formation. If the patient is dehydrated, he or she will have low urine output and therefore the urine can be supersaturated. Urine pH is very important for the formation of some types of stones. For example, low urine pH is favorable to formation of CaOx and uric acid stones while a high urine pH promotes CaP stone formation.
Dietary causes may also generate increased risks of various stones. High sodium intake increases urinary calcium excretion. High oxalate diets, large dose of vitamin C supplements (>1,000 mg/d) will increase urinary oxalate level. High protein diets (> 2.0 g/kg/d) can increase urinary calcium, decrease urine pH and also increase urinary uric acid level [14]. Therefore high protein diets can increase CaOx, and uric acid stone risks. Diuretics, such as furosemide can induce dehydration which can increase risk of supersaturation of solutes.
Environmental conditions such as heat may increase non-renal evaporative skin losses and by doing so they reduce urine volume and increase stone risk [2445464748495051]. The most challenging aspect of encouraging patients to increase their fluid intakes is that they cannot wait for the normal thirst mechanism to urge them to drink because the hypothalamic- pituitary sensors/ neurons lead to increased antidiuretic hormone levels; therefore, the urine becomes more concentrated before the thirst mechanism is triggered and the urine becomes more dilute. One patient education method used is to remind people to drink fluid after each void.
Urine volume: a critical factor
Urine must be supersaturated with solutes to form a crystal, the first step to form a stone. Low fluid intake will lead to low urine output. When urine volume is low, the urine can theoretically be easily supersaturated with various solutes, such as calcium, oxalate, phosphorus, and uric acid. However, there are several inhibitors normally present in the urine to prevent crystallization of these solutes [52535455]. Only if the supersaturation is very high does the crystallization start. The most direct way for patients to decrease risks of supersaturation is to increase the urine volume with oral fluids to above 2.5 L/d of urine volume [56].
Hypercalciuria
Figure 2 shows a model of how idiopathic hypercalciuria occurs. Normal urine calcium excretion is less than 200-250 mg/d. If urine calcium excretion is higher than this, stone risk increases. To evaluate the stone risk, it is necessary to measure serum calcium, urinary calcium, oxalate, urine urea nitrogen (UUN), citrate, magnesium, creatinine, and volume (Table 5). In idiopathic hypercalciuria, the serum calcium level is normal but urinary calcium is high because of increased absorption of calcium from the gastrointestinal tract. The increased absorption of calcium increases the ionized calcium level, decreases parathyroid hormone (PTH) secretion and decreases renal tubular reabsorption of calcium. The increased intestinal calcium absorption can be treated with 1, 25-dihydroxy vitamin D3. There is also evidence of reduced proximal tubular reabsorption of sodium and calcium in patients with idiopathic hypercalciuria, which leads to a negative calcium balance [57]. The combination of a low sodium diet and thiazide diuretics may lower urinary calcium excretion by increasing reabsorption of calcium.
Hyperoxaluria
The most common type of stones are CaOx (75%) and a high urinary excretion of oxalate is a risk factor for them. Dietary sources of oxalate include spinach, rhubarb, beets and some berries. Oxalate is also created from endogenous metabolism of glycine, hydroxyproline and ascorbic acid. A low oxalate diet is recommended for the prevention of CaOx stones; however, a recent study showed that dietary oxalate had little effect on urinary oxalate excretion although vitamin C intake was highly correlated with urinary oxalate excretion [58].
Increased urinary oxalate excretion has also been noted in patients with diabetes [5759]. Patients with IBD have a high prevalence of CaOx stones with hypocalciuria due probably to their negative calcium balance. Negative calcium balance can also cause secondary hyperparathyroidism to maintain normal calcium levels in blood, and a calcium supplement may be effective for preventing CaOx stone risk by decreasing the hyperparathyroidism. The timing of calcium supplements is important and patients should take supplements at the meal time to bind oxalate from dietary sources. Individuals who have had restrictive bariatric surgery have a high risk of hyperoxaluria due to malabsorption and increased reabsorption of oxalate, which may increase hyperoxaluria [2960]. Recent studies by Jiang et al. suggest that enteric colonization with Oxalobacter formigenes, which uses oxalate as a main energy source, reduces the risk of CaOx stone recurrence among individuals whose intakes of calcium were low [61]. In contrast, there is insufficient evidence to support the use of probiotics to reduce stone risk at this time [62].
Hypocitraturia
The urine is usually supersaturated with solutes, especially CaOx; however, the level tends to be less than the 10 times the level of concentration to form the CaOx crystals due to the presence of citrate in the urine. Citrate in the urine binds with urinary calcium to form a soluble compound and this increases the urine pH. CaOx stone formation is favored by a low urine pH; therefore, citrate can help prevent CaOx stone formation. The most common form of citrate prescribed is potassium citrate. The normal value of urinary citrate for males is >450 mg/d and for females >550 mg/d. Renal tubular acidosis and chronic diarrhea can also cause decreased citrate in the urine. However calcium, oxalate and urine pH should be checked before initiation of citrate treatment [63]. If urine pH increases later with citrate treatment, the risk of CaP stone formation rises. In patients who have IBD with high urinary oxalate, and low urinary sodium levels because of malabsorption and gastrointestinal loss of sodium, sodium citrate is more beneficial than potassium citrate, and it should be used. However, sodium citrate can increase urinary calcium excretion and therefore it may increase the risk of CaOx stones.
pH
Urine pH is an important factor in the formation of kidney stones. A low urine pH can promote CaOx and uric acid stones, and a high urine pH can increase the risk of CaP stones. Urine pH is affected by the acid and alkaline ash from the diet, and before the advent of effective urinary acidifying and alkalinizing agents, it was necessary to rely on diet to alter urinary pH, although this could rarely be accomplished effectively. The practice has been largely outdated by the advent of better acidifying and alkalinizing agents. The mineral salt that predominates in foods determines whether the residue or 'ash' is acidic or alkaline. The minerals producing alkaline ash are sodium, potassium, magnesium, and calcium. Acid-forming minerals are sulfur, chlorine, and phosphorus. High animal protein diets which have high purine content and sulfur containing amino acids can reduce urine pH and will lead to an increased risk of uric acid stones. An alkaline ash diet which is high in citrate, mostly from fruits and vegetables, can increase urine pH and citrate excretion. Today alkali therapy is preferable because an alkaline ash diet is difficult to follow for most patients although an alkaline ash urine is preferable for the certain type of stone risk. However, for other stones, the reverse may be true. A high pH without alkali therapy may increase the risk of struvite stones from a UTI.
Uric acid
The prevalence of uric acid stones is about 5% of total kidney stone disease. The main determinant of uric acid stones is urine pH. A low urine pH has more insoluble uric acids concentration; therefore, the risk of uric acid stone is higher. Measurements of urinary calcium, uric acid, and post-prandial urine pH are used to assess the uric acid stone. The average adult consumes about 2 mg of purine/kg/d, which produces 200-300 mg of uric acid daily. Endogenous production of uric acid is about 300 mg/d. In some studies, uric acid excretion is 5.6 mg/kg/d [32] and total excretion of uric acid is less than 800 mg/d. Dietary consumption of purine varies daily among individuals. Kessler et al. conducted a cross-sessional study by using bicarbonate-rich mineral water and various types of juices on uric acid stone formation and found that black current juice decreased uric acid stone risk the most, by increasing the urine pH [6465]. Ingestion of alcohol can also affect urinary uric acid excretion, and excesses should be avoided. If patients have gout, allopurinol is usually prescribed along with low purine diet to reduce blood uric acid and uricosuria [3234].
Dietary risk factors
Several dietary factors can increase risk of the stone formation, including sodium, protein, potassium, calcium, magnesium and other nutrients. These constituents can be modified depending on the types of different stone risks. Foods that produce acid-ash after being metabolized in the body can affect the lowering of urinary pH whereas alkaline-ash foods can increase urinary pH. The specific diets are based on urine pH, urinary uric acid and types of stones (Table 6).
Sodium
Dietary sodium restriction alone decreases urinary calcium excretion [5467]. Proximal tubular calcium reabsorption is increased on a low sodium diet (2,000-3,000 mg/d) and this in turn decreases the SSCaOx. In addition of thiazide diuretics, calcium reabsorption is enhanced and further decreases hypercalciuria. However, addition of thiazide can lead to volume depletion; although ion exchange and volume status will come to the steady state in a few days. If the patient continues to consume a high sodium diet, sodium will reach the distal nephron and increase the excretion of calcium and potassium along with citrate, resulting in a change in the urinary pH that will eventually increase the risk of stone formation. Therefore, after analyzing the 24-hour urine, stone risk is high, prescribing a low sodium diet will help avoid inappropriate thiazide use for patients with CaOx stones. Patients with IBD usually have low urinary sodium levels and low urinary citrate, and so use of sodium citrate instead of potassium is beneficial to improve fluid status from gastrointestinal losses and increase urine volume.
Potassium
Potassium is abundant in most fruits and vegetables. However, if the patient has low urinary citrate and low urine pH, potassium citrate is commonly used along with such a diet to further improve hypocitruria. Monitoring 24-hour urinary excretion of potassium is important to evaluate compliance to diet and medications. Taylor et al. analyzed the 24-hour urine with the Diet Approaches to Stop Hypertension (DASH) diet and found that diets conforming more closely to DASH had decreased risk of stone formation [6869]. Because high DASH score foods are high in potassium, magnesium, and phosphorus, these may increase urine pH, resulting in a decrease in SSCaOx and uric acid in the urine as well as increased urine volume and citrate [6869]. If patients have chronic kidney disease and take angiotensin converting enzyme inhibitors (ACEI) as antihypertensive medications, serum potassium level should be monitored closely.
Protein
There are few markers of 24-hour urine to evaluate dietary protein intake, production and excretion. Urea nitrogen appearance (UNA) and PCR are measurements of daily protein intake that are calculated per kg body weight. In normal healthy steady state, intake of protein can be equivalent to protein catabolism; therefore, PCR determines the nitrogen balance from 24-hour urine urea concentration:
Patients who have acute, or chronic infection are usually malnourished and experience catabolism, and have more nitrogen in the urine. Therefore, this formula should not be used to evaluate protein intake. For patients without active stress of illness, the PCR can guide protein recommendations for patients to prevent further stone risks.
The ammonium (NH4) level should be low in patients who are prescribed alkali therapy or who present with RTA. Monitoring citrate, an indicator of urine acidity, can identify these problems. Patients who take alkali therapy especially with low citrate levels have low urinary ammonium levels with higher pHs and therefore the risk of uric acids or CaOx can be substantially decreased.
High ammonium and sulfate are indicators of a high protein diet, especially one which is high in animal protein [3070]. A high protein diet (>2.0 g/kg/d) can reduce urine pH; therefore, a moderate to low protein diet should be advised (0.8-1.4 g/kg/d). Currently most common and popular weight loss diets promote consumption of large amounts of protein but such a reducing diet is not recommended for the patients who have a history of kidney stones. This high protein diet regimen increases hypercalciuria, lowers pH of urine and increases uric acid levels, which increase kidney stone risk [14]. Massey et al. conducted a study to monitor the effect of stone risk in beef vs. plant protein and concluded that a moderate amount of protein intake of either type had the same effects in reducing CaOx stone risk [71]. The amount of protein seemed to be a more important factor in that study. Recently, an epidemiological study showed that animal protein intake was not independently associated with the incidence of nephrolithiasis among a large cohort of postmenopausal women [72]. However, the evaluation of stone risk varies by individuals and is complicated. Therefore, the recommendation of a usual protein intake remains until the scientific evidence to change this recommendation is provided.
Calcium
Approximately 20% of dietary calcium is absorbed under normal conditions. There is substantial evidence that a higher calcium diet is associated with lower kidney stone formation, because the higher calcium intake will bind oxalate in the gut if it is consumed with meals thereby reducing oxalate absorption. Patients who consumed a diet with a normal calcium intake (i.e., 1,200 mg/d) plus a low animal protein intake had a 51% lower incidence of recurrent stones than patients who consumed low (400 mg/d) calcium diets [20]. Although data to date on taking calcium supplements does not show that they are theoretically effective in reducing stone risk, taking a calcium supplement with meals is beneficial because calcium can bind with the dietary oxalate and thus it is not absorbed.
Magnesium
Magnesium forms a complex with oxalate and decreases SSCaOx in the urine, which can reduce the risk of stone formation [6869]. The DASH diet, which is high in magnesium, showed a decrease in stone risk by increasing pH and lowering SSCaOx [13686973]. Magnesium can also bind with oxalate in the gastrointestinal tract to reduce oxalate absorption; however, a magnesium supplement is not recommended especially patients with chronic kidney disease because magnesium is accumulated in the blood in advanced kidney disease. Decreased urinary magnesium may be a sign of malabsorption, malnutrition, small bowel disease or laxative abuse. Hypomagnesemia is not a risk factor for stone formation.
Vitamin C
Vitamin C is metabolized to dehydroascorbic acid and then converted to oxalate which is then excreted in the urine; therefore, a high vitamin C intake can be a risk for stone formation by increasing endogenous oxalate. A recent observational study showed that consumption of more than 1,000 mg/d vitamin C was associated with a 40% higher risk of stone formation in men than in those who consumed the Dietary Reference Intake (DRI) for vitamin C [74].
Other dietary factors
Citrate consumption can increase urine pH, and also increases citrate concentration in the urine. Citrate also decreases SSCaOx due to its capacity to form a complex with calcium ions and inhibit crystallization of CaOx [63]. However, citrate may increase the risk of CaP stones. A clinical trial conducted by Koff et al. used potassium citrate and lemonade for 21 stone patients, and showed that potassium citrate increased urine pH with increased urinary citrate level but lemonade did not have an effect on urinary pH or citrate levels except for increasing urine volume [75].
Treatment of Kidney Stones
Management in the acute setting
Urgent surgical intervention is indicated in a patient with an obstructed, infected urinary tract, worsening renal function, intractable pain or vomiting or obstruction of a solitary or transplanted kidney. Analgesia is essential and parenteral Non-Steroid Anti-Inflammatory Drugs (NSAIDs: Ketorolac) are as effective as narcotics. NSAIDS are less likely to cause nausea, but should be avoided if the patient has impaired renal function. Pain is due to renal capsule dilatation, and so intractable pain may require decompression of the obstruction. Volume expansion with intravenous fluids is important in correcting the volume depletion that may have occurred from decreased intake and/ or vomiting and it may also increase the likelihood of stone passage by increasing urine production.
If urgent intervention is not required, the treating physician needs to decide if the stone can be passed spontaneously. The likelihood of spontaneous passage decreases as the size of the stone increases and stones >5-6 mm are not likely to pass spontaneously.
Patients who are having repeated stone attacks should be instructed to strain their urine and to submit the stone for composition analysis. Repeated imaging (plain abdominal radiography (KUB) for radiopaque stones and CT for radiolucent stones) is warranted to confirm stone passage. If follow-up imaging reveals no movement after a month, urologic intervention is generally warranted [79].
Surgical treatment
Larger and more proximal ureteral stones are less likely to pass spontaneously and usually require urologic evaluation. If the stone does not pass rapidly, the patient can be sent home with oral analgesia and instructions to return for fever or uncontrollable pain. Most urologists wait a few days before intervening unless there is a possible infection, low likelihood of spontaneous passage or unrelenting pain. Infection in the setting of obstruction is a surgical emergency and mandates emergency drainage.
Extracorporeal shock wave lithotripsy (ESWL) is a non-surgical procedure using shock waves to fragment stones into small pieces which pass spontaneously several days or weeks later. Obese patients may not be effectively treated with ESWL. Cystine stones are very hard and are often not effectively treated with ESWL (Figure 3).
Flexible ureteroscopic stone removal, although invasive, is associated with a better chance of becoming stone free with a single procedure. It does have higher complication rates of ureteral injury or structure, though has become increasingly popular, because of the variety of devices that are available for stone removal including small diameter flexible ureteroscopes, ureteral access sheaths, holmium laser lithotripsy and stone baskets.
Percutaneous nephrostolithotomy is more invasive, but may be necessary for large stones or stones that cannot be removed cystoscopically. It is rare that a patient requires open ureterolithotomy or nephrolithotomy.
Medical and dietary treatment - preventive therapy
A recurrent stone former should undergo an evaluation for a treatable metabolic cause of kidney stones. This is guided by the results of the 24-hour urine collection.
Table 7 summarizes the dietary managements of kidney stones. Fluid intake is an essential component of treatment and should be adjusted so that urine output is greater than 2.5 L/day. Low urine citrate can be corrected using potassium citrate. Table 8 provides some general guidelines for treatment.
Treating calcium stones
Dietary sodium restriction is important as it is associated with a reduction in urine calcium excretion. Thiazide diuretics lead to increased serum calcium levels and reduced urine calcium levels and are therefore used in therapy for patients with hypercalciuria. Oxalate reabsorption in the colon is reduced by the formation of insoluble calcium oxalate. This is very important in therapy because restricting dietary calcium results in less calcium being available in the intestinal lumen to bind oxalate. This leads to increased oxalate absorption and therefore increased urinary oxalate excretion [25]. Table 9 shows the list of high oxalate foods.
The high oxalate foods are considered to be healthy, with high fiber and nutrient dense in vitamins and minerals. Patients who have diabetes, hypertension and high blood cholesterol are often instructed to consume high oxalate foods such as fruits and vegetables. When patients develop kidney stones, they are instructed to change the diet to lower oxalate contents and therefore most patients are confused. The clinical dietitian should be able to advise the patients individualized diet to prevent kidney stone but to keep healthy diet.
Treating uric acid stones
As uric acid is more soluble in an alkaline urine, urine alkalinization is an important part of the treatment of uric acid stones. Patients should decrease their intake of animal proteins which helps decrease uric acid generation. Allopurinol, a xanthine oxidase inhibitor, is used to decrease the formation of uric acid.
Treating cystine stones
There are no specific diet recommendations for cysteine stones except increasing fluid intake. Cystine solubility can be increased by alkalinization of the urine, although solubility only increases when the pH reaches 7-7.5. Thiol containing drugs like Penicillamine and Tiopronin may be given to patients who are unable to comply with increased fluid intake and urinary alkalinization or fail despite it. These drugs increase the solubility of cystine. Tiopronin is better tolerated than penicillamine which is associated with multiple side effects including rash, fever, serum sickness, epidermolysis and membranous nephropathy. Captopril is used because of its sulfhydryl group forms a thiol-cysteine disulfide bond that is more soluble than cysteine. However its efficacy is unclear. Low animal protein diet can lower the stone risk by lowering methionine which is precursor of cystine [84].
Treating Struvite stones
The preferred treatment of struvite stones is surgical removal because they are large. Antibiotic therapy is important and may slow stone growth. It is important to culture stone material to help direct antibiotic therapy. However low sodium diet can help prevention of struvite stone [84].
Conclusion
Kidney stones are common and recur frequently. Calcium oxalate stones are the most common. Urine supersaturation is increased with low urine volume and with increased urinary excretion of calcium, oxalate, phosphate, cysteine or uric acid. Citrate is the most common inhibitor of crystal formation and urinary pH is very important for preventing or treating different types of stones. There are many stone risk factors among which diet is very important one. Urgent stone removal and treatments are done by urology using surgery or ESWL. Medical and dietary treatments are most important ways to prevent recurrence of stone. Consumption of ample fluids is essential, and dietetic advice is helpful.











 XML Download
XML Download