

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Morbid obesity is a serious social problem that decreases the quality of life while increasing the mortality and morbidity rates compared to healthy individuals. In South Korea, as the number of severely obese patients has been increasing each year, the number of subjects undergoing bariatric surgery is also increasing [1]. Bariatric surgery is a very popular option for western obese patients, and it is known to have many positive effects on weight loss and changes in metabolic indices [2]. In order to adapt to sudden changes in dietary quantity and to prevent nutritional imbalance after the surgery, specialized nutritional management is essential. Nutrition research on patients undergoing bariatric surgery is rarely conducted in Korea [3]. Although investigation continues into dietary contributors to obesity, excess energy intake, and, particularly, increased amounts of fat may promote obesity because fat is the most energy dense [4]. But some studies have focused on calorie intake and nuritional deficiency. Thus, we report a case with reviews of literature investigating the changes in fat intake, body fat, and abdominal fat before and after the bariatric surgery.
Case
A 51-year-old man who had an excavator managing job at a construction field, as a head of the household of a multicultural family, had been steadily gaining weight since his 30s. The patient suffered from a herniated disc, gonarthritis, and sleep apnea as his weight reached 106 kg. He lost approximately 13 kg through exercising during 1 year prior to the surgery. When the weight loss slowed down, he visited the Bariatric Surgery Center at Soonchunhyang University at Bucheon Hospital in June 2013 for a surgical consult. At the time of the surgery, his weight was 93.0 kg and BMI was 35.8 kg/m2, which was corresponding to severe morbid obesity. Medical comorbidities included fatty liver and hyperlipidemia.
The patient underwent laparoscopic sleeve gastrectomy on July 11, 2013. He followed up at the hospital before surgery, 1 month, 3 months, and 6 months after the obesity surgery. He underwent examinations for anthropometry, body component, blood test, and dietary survey on each visit. Abdominal computed tomography (CT) was performed 6 months before and after the surgery. Dietary counseling included nutritional assessment, changes in eating behavior, nutrient considerations, weight-loss strategies, motivation, telephone consultation, and nutrition diagnosis. All physicians and a professional nutritionist provided patient education on every visit along with the feedback the test results.
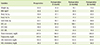
Changes in the patient's anthropometry, body fat, and blood test measurements during the 6 months following the surgery are shown in Table 1. The patient's weight decreased by approximately 20 kg from 93 kg to 73.3 kg, close to his target weight of 70 kg. His body fat decreased from 32.4 kg to 22.2 kg, and body fat percentage decreased from 35.5% to 33.0%. His waist circumference decreased by approximately 20 cm from 114 cm to 93.4 cm. His liver function test decreased to normal levels, which was proven by the decrease in aspartate aminotransferase level to 17 IU/L and an alanine aminotransferase level to 19 IU/L at 6 months after the surgery. His triglyceride level decreased from 215 mg/dL to 104 mg/dL at 6 months after the surgery, while high-density lipoprotein cholesterol level increased from 39 mg/dL to 56 mg/dL.
The abdominal CT scans before the surgery and 6 months after the surgery are shown in Figure 1. The area of the fat has been represented by the green color. The area of subcutaneous fat of patient decreased 28.3% from 293.7 cm2 (A) to 210.5 cm2 (B) after operation. While the area of visceral fat decreased 59.0% from 317.8 cm2 (C) to 130.4 cm2 (D), showing remarkable improvement compared the change of area subcutaneous fat. The visceral-to-subcutaneous fat ratio (VSR) was changed from 1.08 to 0.62 and remained stable after the surgery.
The patient's nutrient intake was investigated using a food recording method and was analyzed using a specialized nutrition analysis program (CAN program ver. 3.0, The Korean Nutrition Society, 2005). The major nutrient intake and fat types are shown in Table 2. Prior to the surgery, the patient consumed excessive amounts of alcohol and meat nearly every day during the week, while his weekend diet mainly consisted of fast food, fried chicken, and fruit. The patient also expressed that he had difficulty of controlling his gluttony. During the first month after the surgery, the patient consumed rice liquid, porridge, and high-protein powder before returning to a regular diet. Three months after the surgery, the patient was able to control his meal portions. As a result, the patient's caloric intake, which was approximately 3,700 kcal before the surgery, was reduced to approximately 900 kcal 6 months after the surgery; and his intake of carbohydrate, protein, and fat also showed dramatic decreases. Cholesterol intake was decreased from 578 mg to 121 mg after the surgery; and his intake of total fatty acid, monounsaturated fatty acid, and polyunsaturated fatty acid was also decreased noticeably. The intake ratio of total fatty acid to monounsaturated fatty acids to polyunsaturated fatty acids showed a positive change with 1:1.1:0.9 at 6 months after the surgery.
After the surgery, the patient no longer had sleep apnea, and no complications or eating disorder were observed during the follow-up care. Moreover, the patient's family members were satisfied and were very supportive to accommodate to his changed body type and lifestyle after the surgery. The patient is still maintaining the effort to keep his current weight by controlling his food intake and exercising.
Discussion
With the increase in obesity and the development of laparoscopic techniques, the frequency of bariatric surgery has increased. The bariatric surgery was first implemented in the 1950s to treat obesity. In this procedure, the sleeve gastrectomy leaves the antrum intact while eliminating the fundus and the main part of the stomach to maintain a normal GI pathway [5]. In the cases abroad, when food intake and lifestyle adjustment accompanied the surgery, significant weight loss of 25-75 kg was observed within 2 years after the surgery [6]. According to Han and Kim [7], patients after sleeve gastrectomy showed weight loss at an average of 20 kg after 6 months and a total of 25 kg within 12 months after the surgery. It is recommended to keep an accurate measurement of the body fat and intra-abdominal fat after the surgery [8]. The study by Weiss et al. [8] revealed a 32% decrease in subcutaneous fat and 35% decrease in visceral fat in patients 6 months after surgery. Furthermore, a numerous studies showed that the obesity surgery improve various health complications such as type 2 diabetes, hypertension, hyperlipidemia, and sleep apnea [9]. In this study, we observed a decrease of 20 kg in weight 6 months after the surgery, with decrease in waist circumference, and improvement in blood lipid tests, as well as a greater decrease in visceral fat compared to subcutaneous fat.
After the bariatric surgery is performed, multi-faced and specialized nutritional management is important [10]. Bothe et al. [11] recommended a daily intake of 800-1,200 kcal to maintain a long-term weight control and reported that the frequent consumption of small amounts along with slow eating habits are necessary to prevent dumping syndrome after the surgery. Moreover, the ingestion of pureed foods for the first 1-2 weeks after the surgery and soft foods there after is recommended to ensure a gradual adjustment. To prevent deficiencies in vitamins and minerals such as calcium, vitamin D, iron, and folic acid, the balanced nutrition and the intake of supplemental nutrition are necessary depending on the patient [12]. The importance of lifestyle changes and continuous management is emphasized to prevent the weight regain. Also, such managements decrease the patients' risk of metabolic diseases [13].
The patient in our study had good compliance during the meal adjustment and controlling period after the surgery. The total energy intake, fat intake, and saturated fatty acid consumption were decreased while polyunsaturated fatty acid consumption was increased. Compared to the study by Kim et al. [14] in Korea, the energy intake of our patient was higher at 6 months after the surgery than the patients who underwent laparoscopic Roux-en-Y gastric bypass, and it was lower than the patients who underwent laparoscopic adjustable gastric banding. But the exact comparison is difficult due to the different surgical methods. A high-fat diet has increased visceral fat accumulation, and whole body and muscle insulin resistance [15]. We evaluated fat mass changes with reduction of fat intake after bariatric surgery. However, this study has several limitations to consider including the smaller sample size and absence of significant difference analysis.
Our patient continued controlling his nutritional intake for weight maintenance even after he reached his target weight. The continuous nutritional guidance is necessary to prevent a long-term malnutrition. Futhermore, subspecialized studies on patients undergoing bariatric surgery are needed, and further efforts are required for the development of a manual for professional nutritional guidelines specific to each surgical method.


 XML Download
XML Download