

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Video capsule endoscopy (VCE) is widely used to examine the small bowel. According to the manufacturers of video capsules, patients should be prescribed a clear liquid diet and fast for 8 h to adequately prepare the small bowel. A meta-analysis illustrated that small-bowel preparation improves the VCE image quality and the diagnostic yield of the examination [1]. However, there is no established optimal regimen to prepare the small bowel for VCE [2]. Small-bowel preparation before VCE is performed to improve the visibility of the small bowel mucosa without affecting the VCE completion rate, capsule gastric transit time (GTT), or small bowel transit time (SBTT) [3,4]. The transparency of the intestinal fluid, which is influenced by the presence of bile, may influence the diagnostic yield of VCE [5]. Although the efficiency of VCE is enhanced by preparatory regimens, the accuracy of VCE is often limited by the presence of dark bile fluid, which results in poor images, particularly in the distal portion of the small bowel [6,7]. Therefore, methods to prevent the presence of bile in the intestinal fluid are important, particularly when attempting to detect distal small bowel lesions or conducting a second VCE study of a patient who exhibited rebleeding after a negative VCE study [8].
Coffee enemas are used in alternative medicine [9,10,11,12]. It has been suggested that the enzymes in coffee stimulate bile excretion [13], which if true suggests that a coffee enema may prevent dark bile fluid accumulation in the distal small bowel. In this paper, we report the findings of a single-blind case-controlled study that evaluated the effects and feasibility of using coffee enemas plus polyethylene glycol (PEG) solution for small bowel preparation compared with a PEG-only preparation. Our hypothesis was that a PEG solution would flush the bile fluid excreted in response to a coffee enema. We compared the VCE images of patients who underwent a coffee enema plus PEG flushing to those of patients who received the PEG solution only. In particular, we focused on assessing the transparency of the intestinal fluid.
Materials and Methods
Study sample
This was a pilot study. We included patients who were referred to Korea University Anam Hospital in Seoul, Korea for VCE between January 2012 and May 2014. Patients were assigned to receive one of two different preparation regimens. The study protocol was approved by the ethics committee of Korea University Hospital, and the study was conducted in accordance with the guidelines of the Helsinki Declaration. Written informed consent was obtained from all patients before the examination. Patients who had incomplete small-bowel examinations, active bleeding, or coagulated blood; those who were receiving oral iron therapy or intensive therapy with fasting and parenteral nutrition; and those who had a history of small intestinal resection were excluded. Patients with , anal or rectal fissures, or rectal prolapses were also excluded. These conditions, if of sufficient severity, could make receiving a coffee enema an extremely painful experience.
Study protocol
All patients were instructed to fast for 8 h before the bowel preparation and VCE examination.
PEG-only group
In the PEG-only group, patients received 2 L of PEG solution (Colyte; Taejun Medical, Seoul, Korea) 2 h before swallowing the video capsule (Pillcam SB2; Given Imaging, Yokneam, Israel).
Coffee enema with PEG group
A split dose of PEG (1 L of the total 2-L dose) was administered before and after the coffee enema. The coffee enema was performed after three defecations following the ingestion of 1 L of PEG. Two or three defecations are required before receiving the coffee enema to improve patients' convenience and enhance the ease of the procedure. The coffee enema fluid was prepared using a coffee maker with two tablespoons of roasted ground coffee (Arabica coffee from Colombia) without any additives and 1 L of distilled water [9]. The brewed coffee was allowed to cool to room temperature and then instilled into the recto-sigmoid colon. The patients were instructed to hold their defecation for approximately 15 min, and then they digested an additional 1 L of PEG after defecation and completion of the coffee enema. VCE was performed within 2 h after the last PEG ingestion was completed.
After bowel preparation, VCE was performed using Pillcam SB2 in accordance with the manufacturer's recommendations. Each subject was equipped with sensor arrays and a data recorder and was instructed to swallow the capsule with a small amount of water. After ingestion of the capsule, each patient remained in the right lateral position for 30 min, after which the patient was free to move around for the remainder of the test. VCE images were recorded for the next 10 h. Patients were then allowed to drink clear liquids and eat light snacks 2 and 4 h after capsule ingestion, respectively.
Assessment of VCE images
Capsule images from each patient were analyzed by a single experienced reviewer (E.K.) who was blinded to the type of bowel preparation. Image quality was assessed using Rapid 5.0 software (Given Imaging). The primary outcome measure was the bowel preparation grade of the small bowel. The secondary outcome measures were feasibility and adverse event related to coffee enemas.
We used the scoring system described by Esaki et al [5]. to assess the quality of the bowel preparation along with the image quality of the small bowel. Video images of the small intestine were separated into three equal segments (proximal, mid, and distal segments) according to SBTT. The terminal ileum was examined to evaluate the effects of coffee enemas on fluid transparency in the distal ileum. If the terminal ileum could not be well differentiated, the image quality of the terminal ileum was assessed using the images taken 10 min before approaching the ileocecal valve. The fluid transparency of each segment and the terminal ileum were initially assessed and graded by reviewing video images at low speed (10 frames/s) under the QuickView mode of the RAPID workstation (Given Imaging). Subsequently, full-length video images were reviewed at maximum speed (40 frames/s) with concurrent manual inspection of individual frames for closer assessment of mucosal visibility under the multiview system. The grade of fluid transparency was determined according to the predominant grade in each segment. The grade of mucosal visibility in each video segment was determined by the duration for which air bubbles or food residues interfered with more than 50% of visualization. The grading system that we used to assess small bowel image quality is described in Table 1.
Evaluation of side effects
After 1 week, patients who had received coffee enemas returned to the clinic for the assessment of adverse events. Hematochezia, abdominal pain, anal pain, fever, and any symptoms related to the coffee enemas were evaluated, and optional laboratory studies were performed for symptomatic patients.
Statistical analysis
Parametric data are expressed as means ± SDs, and these data were compared between groups using the Mann-Whitney U test. Nonparametric data are expressed as frequencies, and these data were compared between groups using Fisher's exact probability test or the χ2 test. p values less than 0.05 were regarded as statistically significant.
Results
Demographic data
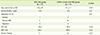
Of the 34 enrolled patients (24 males and 10 females, mean age: 57.7 years, age range: 20-74 years), 17 patients received 2 L of PEG only, and 17 patients received a coffee enema with 2 L of PEG. As shown in Table 2, there were no significant differences in age or gender between the two groups. The bowel preparations and coffee enemas were performed without any significant adverse events. Cecal inspection was achieved in 14 patients who underwent bowel preparation with PEG only (82%) and in 16 patients who were underwent bowel preparation with a coffee enema with PEG (94%).
The indications for CE included obscure gastrointestinal bleeding (total n = 21, PEG only = 11, PEG with coffe enema = 10) and anemia (total n = 4, PEG only = 1, PEG with coffee enema = 3), whereas the other nine subjects were volunteers (PEG only = 5, PEG with coffee enema = 4).
Capsule transit
The gastric transit time (GTT) did not differ between the PEG-only and coffee enema with PEG groups (35.4 ± 49.1 min vs. 26.8 ± 30.3 min, p = 0.39). Similarly, the small bowel transit time (SBTT) did not differ between the two groups (335.2 ± 106.9 min vs. 296.8 ± 86.3 min, p = 0.07).
Image quality
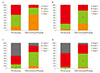
In both groups, the fluid transparency was worsened by bile according to the advance of the capsule in the small bowel. Figure 1 presents a comparison of the fluid transparency during each time segment as determined by the blinded observer. In the mid segment of the small bowel, grade 1 transparency was more frequent in the coffee enema with PEG group than in the PEG-only group (Figure 1B), and in the distal segment, grade 1 or 2 transparency was more prevalent in the coffee enema with PEG group than in the PEG-only group (Figure 1C). Consequently, fluid transparency was better in the coffee enema with PEG group than that in the PEG-only group in the mid and distal segments and the terminal ileum (p = 0.04, p = 0.007, and p = 0.002, respectively, Figure 1). In the proximal segment of the small bowel, the fluid transparency difference did not reach statistical significance (p = 0.1, Figure 1A). Figure 2 shows the VCE images of the two groups.
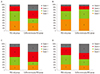
The grades of mucosal visibility due to air bubbles in the two groups were not different in any segment of the small bowel or terminal ileum (Figure 3).
Positive findings
Positive findings were identified in 21 of 34 patients (62%). Multifocal intestinal lesions were found in six patients. Of these 21 patients, 10 (multiple lesions in four) were in the coffee enema with PEG group, whereas the remaining 11 patients (multiple lesions in two) were in the PEG-only group. Consequently, the number of positive findings of VCE was not significantly different between the two groups.
Discussion
Many trials have been conducted to improve the diagnostic yield of VCE [14], which appears to depend largely upon the quality of small bowel images [5]. Bowel preparation using electrolyte lavage solution or simethicone enhances the image quality of VCE [7,15,16]. Bowel preparation with sodium phosphate before CE allows better visualization than overnight fasting alone, and reduces disturbances caused by intraluminal turbid fluid [7,16]. A previous study reported no difference in image quality when bowel preparation was performed using 2 L of PEG versus a 12-h fast [17]. However, subjects who received 2 L of PEG the night before VCE had poor image quality due to the presence of dark bile fluid, even in subjects who received 2 L of PEG. In addition, this previous study was a retrospective study. A meta-analysis found that bowel preparation was more effective at improving image quality than a 12-h fast [1]. Enhanced image quality is believed to improve the rate of detection of lesions and abnormalities.
Although several small bowel preparation methods have been reported, no well-designed prospective controlled studies directly comparing these methods have been performed. When VCE is performed, images are taken for 8-12 h after ingestion of the capsule, and the image quality deteriorates toward the distal ileum compared to that in the proximal jejunum due to the presence of dark bile fluid [18]. Although the control group in this study received 2 L of PEG, turbid fluid that severely obscured vision in the distal third segment of the small bowel and the terminal ileum was observed in over 70% of these patients. Because this type of visual disturbance cannot be controlled by a bowel preparation such as PEG in the distal small bowel, we administered coffee enemas to address this problem and assessed the applicability, safety, and efficacy of this technique.
A number of hypotheses regarding the mechanisms underlying the effects of coffee enemas have been reported. The proponents of coffee enema use believe that the cafestol palmitate in coffee increases the activity of glutathione S-transferase, an enzyme that cause dilatation of bile ducts and excretion of bile through the colon wall, and that the coffee fluid stimulates peristalsis and drainage of bile from the gut [9,10,13]. It has been theorized that the chemicals in coffee enemas cause free radicals to be absorbed by the sulfhydryl (-SH) groups of glutathione in the bile, which thereafter become bile salts that are flushed out of the gall bladder [20]. Based on these reports, we decided to investigate whether the administration of coffee enemas would have the effect on bile excretion. Specifically, we investigated whether the use of coffee enemas would promote the excretion of bile, and if so, whether the released bile could be flushed with PEG to improve the image quality of VCE in distal small bowel segment.
Coffee enemas should be administered before the administration of PEG when preparing for VCE. However, coffee enemas are extremely uncomfortable for patients when the rectum is full of fecal material. Therefore, we first administered 1 L of PEG to promote one or two defecations. The bile excreted due to the coffee enemas was then flushed with an additional 1 L of PEG. A coffee enema rather than an oral dose was utilized in this study because 1 L of coffee extract is difficult to ingest in addition to the customary 2 L of PEG, and the coffee solution itself could impede VCE.
Few complications have been reported following coffee enemas. The majority of the complications previously reported for coffee enemas were cases of proctocolitis caused by thermal injury due to the administration of hot coffee [20,21,22,23]. Dehydration or electrolyte imbalances due to frequent enema use have also been reported [20]. There are two reports of coffee enema-related deaths. One was due to electrolyte imbalance caused by frequent enema administration [24], and the other was due to septicemia in a patient with terminal stage breast cancer and severely compromised hepatic function and immunity [25]. However, the one-time administration of coffee enemas to patients without severe illness typically produces few or no adverse effects [14]. Thermal injury of the rectum can be prevented by controlling the temperature of the coffee enema, and the risks of electrolyte imbalance or septicemia due to frequent enema are not relevant for patients undergoing a one-time procedure for small bowel preparation. To prevent complications, we brewed 1 L of roasted coffee without added flavors (1 L of water and two tablespoons of coffee), allowed the coffee to cool to room temperature, and then administered it to relatively healthy patients. The absorption time of ingested coffee is known to be 30-40 min after fasting. The absorption of a coffee enema is assumed to require a similar amount of time as that for ingested coffee; therefore, we administered an additional 1 L of PEG 30 min after the 15-min coffee enema. In this study, the fluid transparency of the CE images in the control group became poor in the distal segment due to the presence of dark bile fluid. By contrast, all segments of patients who received coffee enemas with PEG flushing were more clearly visualized. The view of the distal ileum was especially clear. Moreover, there were no adverse events in the coffee enema plus PEG group. Therefore, the administration of coffee enemas plus PEG flushing improves the image quality of the distal small bowel. Additionally, coffee enemas plus PEG flushing may be used for retesting capsule-negative patients.
We used the small bowel preparation grade system described by Esaki et al [5] in this study. Previous studies found that the inter-observer agreement between two specialists using this system was relatively high (r = 0.77-0.88), [5] and this grading system is relatively simple. In addition, this grading system can be used to simultaneously assess mucosal visibility and fluid transparency and differentiate between the effects of coffee enemas on bile and poor visibility caused by bubbles and food debris.
This study had some limitations. We did not identify the mechanism of action of coffee enemas and did not determine the relationship between coffee enema administration and bile excretion. Additional large scale prospective controlled studies should be conducted to evaluate the safety of coffee enema use. In addition, the acceptance of coffee enemas among patients also needs to be studied. Ingesting 2 L of PEG plus coffee enema provokes discomfort, potentially reducing compliance with the VCE exam. In addition, future studies with the aim of decreasing the total PEG volume ingested are necessary for its combination with coffee enema. Also, the time interval between last ingestion of PEG solution and capsule exam were not different in 2 study groups, in PEG plus coffee enema group, the time intervals were 2-4 hours shorter than PEG only group. This time interval can be another factor that influence the preparation of distal small bowel.
Conclusion
Coffee enemas administered for small bowel preparation before VCE is feasible and may improve visual disturbance caused by bile in distal small bowel VCE images. Further studies are warranted to evaluate the safety and effectiveness of coffee enemas, as well as to analyze how coffee enemas affect bile excretion.


 XML Download
XML Download