

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Meeting the basic nutritional requirements of the mother while maintaining proper storage of nutrients is essential for the proper development of the fetus within the maternal body [1]. As such, appropriate nutritional management of pregnant women is very important for the growth of the fetus. Recommended macronutrient and micronutrient intake levels for pregnant women are similar to those for healthy nonpregnant women with the exception of those for several vitamins and minerals, including folic acid, iron, and vitamin D, for which, in addition to calories, recommended levels are higher. Inadequate caloric and nutrient intake during pregnancy may lead to anemia, toxemia, and a variety of obstetric complications for the mother, as well as immaturity and neonatal death of the fetus [2,3]. For this reason, particular emphasis is paid on the importance of maintaining a healthy and balanced diet during pregnancy.
Maintaining proper nutrition during pregnancy becomes even more significant when the pregnant women have diabetes. Pregnant women who have been diagnosed with type 2 diabetes mellitus (T2DM) pregestation or who develop gestational diabetes mellitus (GDM) during gestation face increased risk of perinatal complications, including macrosomia, shoulder dystocia, birth injuries, hypoglycemia, and hyperbilirubinemia [4,5]. For these women, proper dietary intake is important for not only providing nutrients for maternal health and fetal growth but also maintaining proper blood glucose and ideal weight gain without ketonenemia [5-8]. The dietary plan for a woman with GDM should be based on the aim of maternal blood glucose control and consideration of the physiological effects that may occur during pregnancy [6]. As exposure to hyperglycemia in early pregnancy increases the risk of fetal complications [9,10], maintaining proper blood glucose control throughout early pregnancy by nutritional management is especially important.
In South Korea, guidance and recommendations regarding clinical nutrition therapy is provided to pregnant women with GDM or T2DM by Korean Diabetes Association and Korean Dietetic Association [11,12]. Nevertheless, few practical national guidelines or educational programs regarding proper nutrition during pregnancy have been developed, and limited research has been conducted into the nutritional intake of women with GDM, leading to lack of understanding of actual nutritional intake. Although several studies have examined the nutrient intake and eating habits of women with GDM [13,14], these studies began collecting data before the pregnant subjects had been diagnosed with GDM, as their study goal had been evaluation of the association between nutrient intake or eating habits and risk of GDM. Thus, the present study aimed to investigate the calorie, macronutrient, and micronutrient intake of pregnant women who have been diagnosed with GDM or T2DM but have received no education from health care practitioners regarding proper dietary intakes during pregnancy. This study could serve as the basis for a proposal to develop nutritional education programs for prevention of the nutrition-related problems that pregnant women with GDM and T2DM are likely to face during the course of pregnancy.
Materials and Methods
Subject selection
The study subjects were selected from pregnant women who were receiving prenatal care at the department of obstetrics and gynecology of a university hospital or a secondary hospital in Seoul, Korea, between June 2008 and May 2010. Those who had been diagnosed with T2DM before pregnancy or had been diagnosed with GDM during pregnancy were asked for the study participation. Diagnosis of GDM had been performed after the completion of two forms of screening and diagnostic testing [15]. Initial screening was performed by measuring the plasma glucose concentration 1-hour after a 50-g oral glucose tolerance test (OGTT). Those with higher values than 140 mg/dL in screening test were considered abnormal and received 100-g OGTT to diagnose of GDM. The criteria of diagnostic OGTT by Americal Diabetes Association is as follows: fasting 95 mg/dL, 1-hour 180 mg/dL, 2-hour 155 mg/dL and 3-hour 140 mg/dL. We identified the women who had two or more the plasma concentrations met or exceeded to the thresholds as GDM. In addition to the inclusion criteria of current pregnancy and diagnosis of GDM or T2DM, all subjects met the inclusion criteria of having knowledge of their diabetic status, not having received any nutrition education regarding glycemic control and proper diet during pregnancy, and being solely responsible for their dietary intake. Of the 132 potential subjects, 7 were excluded because they met one of the exclusion criteria of carrying multiple fetuses and consuming either fewer than 500 kcal/day or more than 4,000 kcal/day. This study was approved by the Seoul St. Mary's Hospital Institutional Review Board (KC10RIMI0190).
Collection of general and clinical data
Data regarding the subjects' background characteristics, personal and family medical history, lifestyle habits and behaviors, and course of pregnancy were collected by experienced research nurses via face-to-face interviews. The collected data included age, occupation, education, physical activity level, alcohol consumption, smoking status, risk factors associated with GDM (history of GDM, macrosomia, polycystic ovary syndrome, and impaired glucose tolerance), and treatment and family history of diabetes. The subjects' height and weight were measured for pre-pregnancy body mass index (BMI) calculated as kg/m2. Appropriate weight gain by gestational age, with the first period ranging from week 0 to week 14, the second period from week 14 to week 28, and the third period from week 28 to birth, on the basis of weight status before pregnancy [16], was determined.
Dietary assessment
Dietary intake data were collected by trained nutritionists using a 24-hour recall method for one day. To ensure that the subjects accurately reported their dietary intake, trained nutritionists instructed them in the use of the 24-hour dietary recall method using aids, such as food models and photographs, to improve accuracy. The nutritionists also asked the subjects whether the meals that they recorded by the 24-hour recall method were similar to the meals that they had eaten after being diagnosed of GDM. Intake of nutritional supplements was not recorded or included in the analysis. The CAN Pro 3.0 (Korean Nutrition Society, Seoul, Korea) was used to analyze nutrient intake of the study subjects.
The regularity of intake and distribution of caloric and carbohydrate intake among meals and snacks throughout the day were determined. Individual caloric recommendations were calculated in consideration of pre-pregnancy weight status (underweight, normal, overweight, or obese) and amount of weight gain during pregnancy (within normal range or excessive) [11]. Nutrient intake recommendations were determined according to the recommended nutrient intake (RNI) of Korean Dietary Reference Intakes (KDRIs) for pregnant women [17]. The appropriate carbohydrate:protein:fat ratio was set at 45:20:35 [11] of caloric intake according to the education guide for diabetes of Korean Diabetes Association and compared with the actual ratio of the subjects. Qualitative measurement of nutrient intake was performed by determination of the nutrient adequacy ratio (NAR), the mean adequacy ratio (MAR), and the index of nutritional quality (INQ).
NAR = nutrient intake of an individual / RNI of the nutrient
MAR = sum of the NAR for each nutrient / number of nutrients
INQ = amount of nutrients in 1,000 kcal / RNI in 1,000 kcal
Statistical analysis
The collected data were analyzed using the Statistical Analysis System ver. 9.1 (SAS Institute, Cary, NC, USA). Subjects were divided into a group that had been diagnosed with GDM during pregnancy and a group that had been diagnosed with T2DM before pregnancy. The results were expressed as mean, standard deviation, frequency, and the percentage values. Baseline characteristics and nutrient intakes were first assessed for normality and then compared between groups using the Fisher's exact test or Wilcoxon rank-sum test of independence.
Results
General characteristics of study subjects
Table 1 shows the general characteristics of the study subjects according to diabetic status. As can be observed, the mean age and gestational week were 32.9 years and 26.2 weeks for the GDM group and 31.6 years and 11.2 weeks for the T2DM group. The pregestation BMI of the GDM and T2DM groups was 23.3 and 25.7 kg/m2, respectively, and the percentage of subjects with weight gain above the recommended level during pregnancy was 21.6% and 42.9%, respectively.
Regularity of meal and snack consumption
Table 2 shows the regularity of the meal and snack consumption of the subjects. More than 90% of all subjects consumed 3 meals a day, and approximately 35% consumed 3 snacks a day (one each in the morning, afternoon, and evening). The percentage of total calories consumed at breakfast, morning snack, lunch, lunch snack, supper, and evening snack was 21.4%, 5.4%, 28.9%, 9.9%, 28.7%, and 5.7%, respectively, for the GDM group and 24.2%, 2.7%, 28.3%, 7.9%, 33.5%, and 3.4%, respectively, for the T2DM group. Both groups consumed a relatively high percentage of carbohydrates at breakfast (GDM and T2DM, 23.1% and 24.9%, respectively), and a relatively low percentage at snacks. Women with GDM had lower proportion of carbohydrate intake at dinner than did women with T2DM (27.8 ± 8.2 vs. 33.7 ± 11.1, p = 0.043).
Assessment of micronutrient intake levels
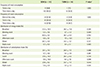
Table 3 shows the subjects' actual caloric and nutrient intake levels compared with the recommended levels. Caloric intake of the GDM and T2DM groups was 1,596.6 kcal, 86.1% of the recommended level, and 1,408.2 kcal, 91.4% of the recommended level, respectively. Women with GDM had higher intakes of protein (p = 0.043), fat (p = 0.005), calcium (p = 0.0.019), zinc (p = 0.009), vitamin B1 (p = 0.0.008) and vitamin B2 (p = 0.001) than did women with T2DM. While the vitamin A and C, sodium intake of both groups exceeded recommended levels, the calcium, iron, zinc, niacin, vitamins B1, vitamin B2, vitamin B6, and folic acid intake of both groups was less than the recommended levels. A particularly notable finding was that iron and folic acid intake was less than 60% of the RNI.
Assessment of macronutrient intake levels
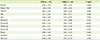
Figure 1 shows the percentage of calories from carbohydrate, protein, and fat intake. The GDM and T2DM groups obtained 56.6% and 63.6%, respectively (p = 0.012), of their calories by carbohydrate intake, which exceeded (125.8% and 141.3%, respectively) the recommended levels. In contrast, the GDM and T2DM groups obtained 17.4% and 16.6%, respectively, of their calories by protein intake, which were lower (87.0% and 83.0%, respectively) than the recommended levels. Interestingly, the GDM and T2DM groups obtained only 26.0% and 19.7%, respectively, of their calories by fat intake, which were far less than the recommended intake of 35%, and this trend was more pronounced in T2DM women (p = 0.006).
Assessment of micronutrient intake levels
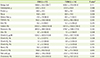
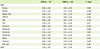
Table 4 shows the NAR and MAR values and Table 5 shows the INQ values for the GDM and T2DM groups. The NAR values, indicators of the ratio of nutrient intake levels compared to the recommended levels, for all nutrients and calories for both groups were below 1, as were the MAR values (GDM group, 0.73 and T2DM group, 0.65, p = 0.045). The INQ values of the GDM group were greater than 1 for dietary fiber, zinc, vitamin A, vitamin B6, and vitamin C, but were less than 1 for the remaining 7 nutrients, indicating intake values lower than recommended levels despite adequate caloric intake. None of the INQ values of the T2DM group exceeded 1 except those for vitamin A and vitamin C, indicating adequate intake of only these 2 nutrients. The INQ values of calcium (p = 0.007), zinc (p = 0.003), vitamin B1 (p < 0.001), vitamin B2 (p < 0.001), and vitamin B6 (p = 0.010) was higher in the GDM groups.
Discussion
The present study aimed to investigate the caloric, macronutrient, and micronutrient intake levels of pregnant women with GDM or T2DM who had not received dietary advice regarding proper meal planning during pregnancy by professionals specially trained for this purpose. Such investigation is important because ensuring adequate intake of calories and nutrients without increasing blood glucose levels or causing excessive weight gain is very important for preventing maternal and fetal complications in this population [4,6,7]. Caloric recommendations for pregnant women with diabetes are based on standards for appropriate weight gain during pregnancy, with certain caloric restrictions recommended for those who are obese or overweight [6-8]. Until the American Diabetic Association (ADA) first recommended caloric restriction for obese patients with GDM in 2000 [18], the recommended caloric intake for women with GDM was similar to that of healthy pregnant women. Based on observation that hyperglycemia can be improved without increasing ketonuria if appropriate weight gain is maintained [6,7], the current recommendation for obese women with GDM is to restrict calories 30% to 33% fewer than the RNI for healthy pregnant women. In South Korea, women with GDM are advised not to increase caloric intake during the early stage of pregnancy, and then to increase intake during the mid and late stages of pregnancy according to their individual situation [11,12]. Women with pregestational diabetes are advised to consume an additional 300 kcal/day during the mid and late stages of pregnancy, depending on their status [12].
No specific recommendations regarding caloric restriction for obese or overweight pregnant women have yet been established. However, the findings of national studies of GDM patients, which reported a high mean pre-pregnancy BMI of 23 to 25 kg/m2 [13,14,19-21], and the findings of the present study, in which approximately 50% of the subjects were overweight or obese, suggests the need to establish recommended caloric intake levels for GDM patients. Accordingly, this study estimated the appropriate caloric intake of the subjects based on not only consideration of existing recommendations but also pre-pregnancy weight and weight gain during pregnancy. Based on these considerations, the caloric intake levels of the GDM and T2DM groups were determined to be 1,597 and 1,408 kcal/day, respectively, which are 86.1% and 91.4%, respectively, of the recommended intake levels for subjects. Few studies of the nutrient intake of women with GDM have been conducted in South Korea. Of the few that have, a case-control study conducted to identify the association between dietary habits and nutrient intake levels reported that the average caloric intake of the GDM subjects was 1,959 kcal/day [14]. It is difficult to make a comparison with the results of this study, because they measured caloric intake using a food frequency questionnaire. Using a 24-hour recall method, Chang et al. [13] and Park [19] found the mean daily caloric intake levels of their GDM subjects were approximately 2,300 and 1,850 kcal, respectively, higher than the mean intake level (1,596 kcal) of the subjects in this study. However, it is also difficult to compare these results, considering the differences in some data collection procedures. The reason why energy intake was reported to be less than recommended values in this study is thought to be due to reduced amount of meals by doctor's advice or in concerns about weight control and blood glucose levels after being diagnosed with diabetes. Dietary intake without professional advice regarding appropriate meal planning in pregnant women with GDM or T2DM is never desirable because it can invoke diabetic ketoacidosis during pregnancy, which pose a great danger to both the mother and fetus. [22,23]. An important consideration is that both the fetus and placenta require large amounts of maternal glucose as a major source of the energy in the second and third trimester, resulting in reduction of maternal glucose level and increase in free fatty acid production and ketone generation in the liver [22]. Given that most women with GDM are diagnosed with the disease after mid-pregnancy, proper training of medical professionals is needed to prevent these risks.
Management of carbohydrate intake of pregnant women with GDM and T2DM is important for postprandial glucose control [4,24]. While several observational and non-randomized studies of GDM patients reported that the percentage of total calories obtained by carbohydrate intake was 30% to 60% [7], the present study found that it was 56.6% and 63.6% in the GDM and T2DM groups, respectively. In 2002, the ADA recommended that carbohydrate intake levels for GDM patients be limited to 35% to 40% of total calories [26], although a recent report recommended it be restricted to 40% to 45% of total calories [26].
It is well known that maternal hyperglycemia stimulates insulin secretion of the fetus through the placenta, a phenomenon that acts like fetal growth factor to increase the risk of macrosomia [4]. The recommendation of 2004 on nutrition therapy for GDM reported that despite the claims of previous studies of improved glucose level of mothers thanks to low-carbohydrate meal, there were few grounds of effect of nutritional treatment on long-term health of mothers and perinatal complications in the current status [7]. Other studies have suggested that intake of low levels of carbohydrates on a regular basis to regulate blood glucose, in conjunction with caloric control and insulin therapy, can reduce the risk of macrosomia [24]. The recent hyperglycemia and adverse pregnancy outcomes (HAPO) study, which conducted glucose tolerance testing of 20,000 pregnant women without diabetes, reported a strong positive association between maternal glucose levels and both fetal body fat status and pregnancy complications [27,28]. For women who have been diagnosed with T1DM or T2DM before pregnancy, maintaining appropriate blood glucose levels via provision of a treatment plan that includes education regarding proper meal preparation is very important, as exposure to high maternal blood glucose levels in early pregnancy may increase the risk of fetal central nervous system and musculoskeletal system disorders and cardiovascular disease [9,10].
For both the GDM and T2DM groups in this study, carbohydrate intake levels as a percentage of calories were above recommended levels while protein and fat intake levels as a percentage of calories were below recommended levels. Specifically, the protein and fat intake levels of the GDM group were only 17.4% and 26.0%, respectively, and those of T2DM group only 16.6% and 19.7%, respectively, compared to the recommended levels of 20.0% and 35.0%, respectively. These findings, which accord with study of Park et al. [20] in GDM patients, suggest that pregnant women with GDM or T2DM be advised to reduce their carbohydrate intake and increase their protein and fat intake, and that women with pre-gestational diabetes be provided with dietary education that emphasizes glucose control during the early stage of pregnancy. When studying the effectiveness of such education, the women's compliance with the recommendations should be considered separately from their understanding of the education provided, as Park et al. [20] found that the subjects did not comply with the recommendations provided during training (i.e., obtaining 52% vs. 45% of their calories from carbohydrates and 27% vs. 35% from fat).
The intakes of nutrients other than macronutrients and calories were evaluated based on the recommended levels [17] for pregnant women of Dietary Reference Intakes for Koreans. Most nutrients did not meet the RNI, and this result is thought to have been partly caused by the low calorie intake. However, ruling out the effect of caloric intake, the INQ values obtained in the present study indicate that the actual intake levels of the GDM group were lower than the recommended levels for all micronutrients except for dietary fiber, zinc, vitamin A, vitamin B6, and vitamin C. Conversely, those of the T2DM group, who had a higher caloric intake ratio than the GDM group, were lower than the recommended levels for all micronutrients except for vitamin A and vitamin C. As the mean INQ values for most micronutrients were less than 1, indicating that the micronutrient intake levels did not meet recommended levels in spite of consumption of sufficient calories, it can be concluded that the dietary quality of the study subjects was not adequate.
With the exception of the values for vitamin A and vitamin C, for which intake levels exceeded the recommended levels, the NAR values for micronutrients were less than 1 for both groups. Because there was no quality assessment study of diet for pregnant women with GDM or T2DM, it is not possible to compare the current study findings with previous studies. In present study, INQ, NAR, and MAR values of subjects indicate that their meal quality was inadequate, suggesting the need to provide them with education regarding meal planning and meal quality as well as proper caloric and carbohydrate intake.
As for all patients with diabetes, eating regular meals is a basic principle of dietary therapy for pregnant women with diabetes. Most sets of dietary recommendations for GDM patients recommend consumption of small meals and 2 to 4 snacks throughout the day for adequate glycemic control [6,12,18,25]. Most study subjects appeared to eat 3 times a day, and 36% consumed a morning, afternoon, and evening snack. Although consuming an evening snack is recommended for pregnant women with GDM and T2DM to prevent night-time hypoglycemia and ketosis [6,12], only 64.9% and 78.6% of the GDM and T2DM groups, respectively, consumed an evening snack (data not shown).
The Korean Dietetic Association recommends restriction of carbohydrate intake at breakfast for GDM patients to prevent a sudden rise in blood glucose. Specifically, it recommends consuming 10% of carbohydrates at breakfast, 20% to 30% at lunch, 30% to 40% at dinner, and 30% from snacks [12]. However, the GDM and T2DM groups consumed 23.1% and 24.9%, respectively, of their carbohydrates at breakfast, more than 200% of the recommended levels, and a relatively lower percentage from snacks, indicating the need to adjust their carbohydrate intake at breakfast.
Several aspects of the study sample and dietary measurements may limit the generalizability of the findings. Regarding the sample, only a small number of T2DM subjects were examined, and all the subjects had a relatively higher educational level compared to those in previous studies of GDM. However, as stratified analysis for education revealed that highly educated subjects tend to consume higher quality meals, it is unlikely that the parameter of education meaningfully distorted the results. Regarding dietary measurements, the recorded nutrient intake levels may not have accurately reflected the actual intake levels because nutrient intake measurement was conducted using a 24-hour recall method for one day. However, all GDM subjects except for one woman responded "yes" when asked whether a meal that they had consumed was similar to the meal that they typically consumed, indicating that they had not changed their dietary habits in reaction to concern about blood glucose control. Another measurement limitation was that nutrient intake via nutritional supplements was not considered. Given that most pregnant women take supplements containing iron and folic acid, additional consideration was required in meal quality assessment through micronutrient. Although many studies reported that pregnant women with GDM and T2DM increase maternal and neonatal risks [4,5], we could not show the results related to pregnancy outcomes because this study was planned as cross-sectional design.
Conclusion
The results of the present study indicate that women diagnosed with GDM during pregnancy or T2DM before pregnancy tend to have inadequate micronutrient intake and unbalanced macronutrient intake when they are not provided with nutritional education by experts specially trained for this purpose. Based on these results, it is strongly recommended that this population be provided with appropriate nutritional education before and during pregnancy to prevent maternal and fetal perinatal complications and post-gestational diabetes, obesity, and cardiovascular diseases.


 XML Download
XML Download