

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Meningiomas are tumors that arise from meninges of the brain and the spinal cord, and the most common intracranial neoplasm constituting 36.7% of all primary brain tumors in United States and 37.3% in Korea [12]. The World Health Organization (WHO) categorizes meningiomas into three grades; grade I as benign meningioma; grade II as atypical meningioma; and grade III as anaplastic meningioma based on histopathological criteria [3]. The majority of meningiomas (>80%) are WHO grade I in which complete surgical resection results in prolonged disease free survival or cure. Among these subtypes, atypical meningiomas are reported to account for 20–35% of all meningiomas and represent an intermediate subtype between benign and anaplastic meningiomas in the WHO classification [45]. The number of grade II meningiomas increased when WHO 2007 classification (30%) was used compared with previous edition, mainly because of the definition of brain-infiltrating meningiomas as atypical meningioma [5].
Although benign meningiomas (WHO grade I) are generally slow growing and have a low recurrence rate after grosstotal resection, atypical meningiomas are more locally aggressive and demonstrate more rapid tumor progression [6]. Therefore, despite initial surgical resection often accompanied by radiotherapy, atypical meningiomas frequently recur and require re-treatment primarily with re-resection or re-irradiation; the literature suggests they have a 5-year recurrence rate of approximately 40% in the absence of postoperative radiotherapy [78]. According to the National Comprehensive Cancer Network (NCCN) guideline for recurrent WHO grade II meningioma, repeated surgical resection is recommended if accessible. However, in surgically inaccessible cases, further radiotherapy if possible regarding the radiation oncology management or systemic chemotherapy with hydroxyurea, α-interferon, or somatostatin analogue are suggested based on consensus expert opinion regarding the medical oncology management [910]. However, these recommendations are based upon a comparatively small literature treating patients with surgery and radiation therapy for refractory meningiomas [111213]. Even, in the new guideline of NCCN for WHO grade II meningiomas (version 1. 2016), adjuvant treatment with hydroxyurea is not mentioned as therapeutic option for the recurrent or progressive disease (PD) in surgically inaccessible tumors and the patients who cannot undergo further radiotherapy.
In 2000, we started to manage the residual atypical meningioma as WHO grade II meningioma with hydroxyurea or radiotherapy after incomplete surgical resection according to the NCCN guideline based on previous traditional and historical literatures. This retrospective case series of 55 atypical meningiomas which were resected incompletely represents the comparative experience in management with adjuvant hydroxyurea chemotherapy or radiotherapy at single institute. In the present study, we aimed to investigate the clinical results of adjuvant chemotherapy with hydroxyurea and compare the results with those of postoperative radiotherapy after incomplete resection of atypical meningioma, especially in terms of progression-free survival (PFS). In addition, we estimated the side effect of adjuvant hydroxyurea chemotherapy for the incomplete resected atypical meningiomas, also investigated clinical and radiological prognostic factors related to the PFS.
MATERIALS AND METHODS
Patient collection
The retrospective study protocol was approved by the Institutional Review Boards of our hospital (2016-SCMC-054-00). We conducted a retrospective case study and clinical review of the 412 meningioma patients who had been surgically treated by Dr. KH Kim and Dr. YZ Kim at the Department of Neurosurgery in the period from January 2000 to December 2014. All patients had undergone radical surgery and histopathologically diagnosed. Among these cases, we selected the 84 tumors that met the diagnostic criteria for atypical meningioma, as outlined in the 2016 WHO classification [6]; brain invasion joins a mitotic count of 4 or more as a histological single criterion and additive criteria of 3 of the other 5 histological features such as spontaneous necrosis, sheeting (loss of whorling or fascicular architecture), prominent nucleoli, high cellularity and small cells (tumor clusters with high nuclear: cytoplasmic ratio) [3].
The following patients were excluded: 1) those with recurrent atypical meningioma after treatment for a previous benign meningioma; 2) those with multiple intracranial meningiomas, because of the difficulty in evaluating treatment response; 3) those with spinal cord meningioma; 4) those who had undergone preoperative radiotherapy for tumor; and 5) those with ≤12 months of follow-up due to follow-up loss.
Patient sex, age at the time of surgery, symptoms at diagnosis, tumor location and size, extent of resection, histological grade, use of postoperative radiotherapy or chemotherapy, duration of follow-up, and recurrence/progression were retrospectively reviewed for each patient by using the medical records.
Radiological findings
Tumor size was defined as the largest tumor diameter rounded to the nearest centimeter on gadolinium-enhanced T1 weighted MR images before the initial surgery. Peritumoral edema was estimated by the longest distance from the margin of the tumor on fluid-attenuated inversion recovery (FLAIR) images. The locations of tumors were divided into convexity and nonconvexity groups. The extent of resection was categorized as either complete or incomplete. Complete resection was defined as Simpson grade 0 or I, and incomplete resection was defined as Simpson grade II–V. The extent of resection was estimated not only during the operation itself but also on MRI, which was performed immediately after surgery. Recurrence was defined as the presence of new tumor in patients with a completely resected tumor, as judged on the first postoperative MR image, and progression as evidence of new growth of an incompletely resected tumor on serial postoperative MR images compared with the immediate postoperative MR images. All patients had undergone preoperative MRI. Baseline postoperative MRI was performed immediately after surgery to evaluate the residual mass and then at 3- or 6-month intervals within the first 2 years. To assess tumor recurrence/progression, serial MRI was performed at 1-year intervals in the patients, but if mass-related symptoms or focal neurological signs developed, MRI was performed immediately. Two neuroradiologists individually conducted radiological reviews to characterize tumors and to determine the presence of a recurrence/progression without any clinical or pathological information on the patients.
Therapeutic strategies for incompletely resected atypical meningioma
All the patients with incompletely resected atypical meningioma were considered to receive the adjuvant treatment after surgery as soon as possible. Before 2009, NCCN guideline contained the adjuvant chemotherapy using hydroxyurea for the incompletely resected atypical meningioma, but this treatment modality dropped out in NCCN guideline for the treatment of these tumors from 2009. Therefore, we recommend mainly hydroxyurea chemotherapy on the adjuvant purpose in all patients with atypical meningiomas that were incompletely resected before 2009. However, we did not treat the adjuvant chemotherapy using hydroxyurea in those patients at all from 2009.
Inclusion criteria for the adjuvant chemotherapy with hydroxyurea in the patients with incompletely resected atypical meningioma were as follows; 1) those with histologically proven atypical meningioma, 2) chemotherapy and radiotherapy naïve patients, 3) those with a Karnofsky performance status better than or equal to 60, 4) those with a life expectancy greater than 3 months, 5) those with adequate hematologic, renal and hepatic functions, and 6) those without serious concurrent medical illnesses or active infection.
In cases of recurrent/progressive atypical meningiomas, reoperation should be considered as the first choice. Stereotactic radiosurgery was an alternative treatment modality for small or surgically inaccessible meningiomas and in patients of advanced age or with a high operative risk. Patients who underwent incomplete resection of the tumor were treated with 3D conformal and intensity modulated radiotherapy. Total irradiation dose ranged from 50 Gy to 60 Gy (1.8–2.0 Gy per fraction a day, 5 fractions a week), depending on the decision of the radiation oncologist. Stereotactic radiosurgery dose ranged from 12 Gy to 18 Gy (median 14 Gy).
Hydroxyurea chemotherapy
Hydroxyurea (Hydrin®; Korean United Pharm Inc., Seoul, Korea) was administered orally for 28-consecutive days (1,000 mg/m2/day divided twice per day or rounded to the nearest dose level based on availability of hydroxyurea capsule size) every 4-weeks (operationally defined as a cycle of therapy). Hydroxyurea was prescribed in a routine practice, and no pharmaceutical sponsorship was provided in the conduct of this study. No premedication was required with oral hydroxyurea. Concurrent medications included non-enzyme mediating anti-epileptic drugs (46 patients), enzyme mediating anti-epileptic drugs (22 patients), analgesics (35 patients), dexamethasone (15 patients), anti-constipation medication (11 patients), anti-hypertensive drugs (10 patients), anti-diabetic drugs (7 patients), anti-cholesterol drug (5 patients), and anticoagulants (2 patients).
Administration of hydroxyurea was repeated every 28 days (4-weeks) provided that all toxicity from the previous cycle had resolved. If recovery had not occurred by day 28, the subsequent cycle of hydroxyurea was delayed until recovery. All toxicities including hematologic due to hydroxyurea chemotherapy were rated retrospectively according to the Common Terminology Criteria for Adverse Events version 4.0.
All patients underwent brain MRI for the base control images within 2 weeks of starting hydroxyurea administration. Blood counts were obtained on day 1 of each hydroxyurea cycle (or more often if clinically indicated), neurologic examination was performed every 4 weeks, and gadolinium-enhanced brain MRI was performed after every 3 cycles of hydroxyurea chemotherapy (i.e., every 12 weeks). Modified neuroradiographic response criteria as defined by Macdonald et al. [14] were used; complete response (CR), complete resolution of the enhancing tumor volume, and an improved or normal neurological examination without steroid medication; partial response (PR), greater than 50% reduction of the enhancing tumor volume and a stable or improved neurological examination on stable or decreased doses of steroid; stable disease (SD), less than 50% reduction or 25% growth of enhancing tumor volume without a significant change in the neurological examination on stable or decreasing doses of steroids; and PD, greater than a 25% increase of the enhancing tumor volume. All neuroradiography was reviewed by 2 neuroradiologists (Kim and Sunwoo) blinded to treatment. In patients with radiographically SD, PR or CR, 3 additional cycles of hydroxyurea were administered and repeat MR was performed. Patients were continued on hydroxyurea therapy until documentation of PD at which time patients discontinued hydroxyurea and were either monitored or offered alternative therapy. Alternative meningioma-directed therapy such as radiotherapy for the radiotherapy naïve patients and repeated surgery (or no additional therapy) was offered to patients that radiographically progressed.
Statistical analysis
Differences between subgroups were analyzed using the Student t-test for normally distributed continuous values and the Mann-Whitney U-test for nonnormally distributed continuous values. The chi-square test was used to analyze categorical variables. PFS was defined as the time from the first day of treatment with hydroxyurea until progression or death, and calculated according to the Kaplan-Meier method, and comparisons between groups were performed using log-rank tests. Variables found to be significantly associated with the progression of atypical meningiomas in the univariate analyses were then subjected to multivariate analyses. Moreover, several additional variables that have been associated with the progression of atypical meningioma in the literature and that we have been interested in were also subjected to multivariate analysis. In the multivariate analysis, the Cox proportional- hazards regression model was used to assess the independent effects of specific factors on the tumor progression rate and to define the hazard ratios for significant covariates. Two-sided p values below 0.05 were considered statistically significant. SPSS version 12.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis.
RESULTS
Characteristics of patients and tumor
From a total of 84 atypical meningioma cases in the defined study period, 55 atypical meningiomas (65.5%) were resected incompletely, which were eligible for our analysis. There were 26 males and 29 females. The mean age at surgery for these patients was 56.8 years (range 26.4–87.2 years). Fifty-three of the patients (96.4%) had clinical symptoms before diagnosis; the most frequent chief complaints at presentation were headache [27 cases (49.1%)], seizures [11 cases (20.0%)], focal neurological deficit such as motor weakness and dysphasia [10 cases (18.2%)], and altered mentation [5 cases (9.1%)] (Table 1).
Twenty-three tumors (41.8%) were located in the convexity regions and another 32 (58.2%) in the nonconvexity regions. The mean maximal tumor diameter was 4.3 cm (range 2.4–8.3 cm), and the mean extent of peritumoral edema was 2.1 cm (range 0.0–5.5 cm) (Table 1).
In terms of histological markers for proliferation, the mean Ki67 index was 6.7% (range 0.0–8.8%), mitotic number was 7.4/10 high-power field (HPF) (range 4–11.2), and p53 expression was 21.2% (range 4.0–37.3%) (Table 1). Extent of resection was as follows; 23 tumors (41.8%) were resected in Simpson grade II, 25 tumors (45.5%) in Simpson grade III, and 7 tumors (12.7%) in Simpson grade IV (Table 1).
After surgical resection, 24 patients (43.6%) were treated with hydroxyurea for adjuvant chemotherapy (group A), 20 patients (36.4%) underwent conventional radiotherapy (group B), and 11 patients (20.0%) received conservative treatment (group C). There were no significant differences of the clinical and radiopathological characteristics among three groups (Table 1).
Tumor progression
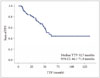
The mean follow-up time from the date of resection was 56.5 months (range 12.4–134.6 months). During follow-up, 25 patients (45.5%) presented with progression, all cases occurring more than 1 year after surgery (Fig. 1). The mean PFS was 30.9 months (range 6.4–62.3 months). The actual 3- and 5-year PFSs were 72.7% and 56.4%, respectively. All progression occurred at the original site of primary resection, and there was no distant metastasis extracranially.
In group A, the mean 25.6 cycles of hydroxyurea were treated for the patients (range 12–64 cycles). Dose of hydroxyurea was 1,000 mg, which was equal to the entire patients due to the dose of the capsule. There were 1 (4.2%) partial remission, 15 (62.5%) SD, and 8 progressions (33.3%) (Table 2). Among total 615 cycles, there were 97 (15.8%) cases of grade 1 adverse effect, 40 (6.5%) cases of grade 2 adverse effect, and 14 (2.3%) cases of grade 3 adverse effect. However, there was no case of grade 4–5 adverse effect (Table 3). Most common adverse effect was hematologic events; among 82 (13.3%) hematologic adverse effects, there were 40 (6.5%) cases of anemia, 25 (4.1%) cases of neutropenia, and 17 (2.7%) cases of thrombocytopenia, respectively. Of the tumors with progression, mean PFS was 46.2 months (range 28.6–62.3 months). After progression, 5 (62.5%) patients underwent adjuvant radiotherapy, 1 (12.5%) patient was treated with repeated chemotherapy using other cytotoxic regimen, and another 2 (25.0%) patients received conservative treatment.
In group B, 7 (35.0%) patients experienced the progression of disease. Mean PFS was 40.4 months (range 25.6–53.2 months). In group C, 10 (90.9%) patients did the progression of disease. Mean PFS was 11.9 months (range 6.4–22.6 months).
Univariate analysis of factors predicting progression
In terms of clinical characteristics, the surgical extent was associated with the progression of the tumor; the p value was 0.048 in Simpson grade II versus III, and 0.004 in Simpson grade II versus IV. Additionally, therapeutic modality of adjuvant treatment was also associated with the progression; the hazard ratio (HR) of the conservative care over the hydroxyurea chemotherapy was 8.64 (95% CI 5.04–12.24; p<0.001). Other clinical factors such as age, gender, seizure, location, and size of the tumors were not associated with progression of the tumors which were resected incompletely (Table 4).
Histopathologically, the known proliferative markers such as high Ki67 index (HR 3.64, 95% CI 2.16–5.12; p=0.026), higher number of mitosis (HR 4.23, 95% CI 3.22–5.24; p=0.012), and more expression of p53 (HR 2.79, 95% CI 1.69–3.89; p=0.041) were also associated with the progression of the tumors (Table 4).
Multivariate analysis of factors predicting progression
Multivariate analysis using Cox proportional hazard regression analysis showed that the following factors were independently associated with a higher rate of progression: 1) surgical extent (HR 3.107 and p=0.043 in Simpson grade IV versus III, HR 5.282 and p=0.006 in Simpson grade IV versus II, and HR 2.545 and p=0.047 in Simpson grade III versus II) (Table 5); 2) adjuvant therapeutic modality after surgery (HR 6.344 and p=0.002 in conservative treatment versus radiotherapy, and HR 7.182 and p<0.001 in conservative treatment versus hydroxyurea chemotherapy) (Table 5); 3) proliferative index (Ki67 ≥6% versus <6%, mitosis number ≥8/10 HPF versus <8/10 HPF, and p53 expression ≥20% versus <20%) (Table 5). Kaplan-Meier survival analysis for PFS also showed statistically significant differences in surgical extent, adjuvant therapeutic modality, and proliferative markers (Fig. 2).
DISCUSSION
The purpose of this retrospective study was to estimate the efficacy of the adjuvant chemotherapy with hydroxyurea and compare the results of postoperative radiotherapy after incomplete resection of atypical meningioma, especially in terms of PFS. To the best our knowledge, there is no result reporting the comparative and comprehensive outcome between adjuvant radiotherapy and hydroxyurea chemotherapy for this unique condition of incompletely resected atypical meningiomas due to their rarity. Most clinical trials using hydroxyurea were aimed at the patients with WHO II/III meningiomas which were recurrent or refractory to the radiotherapy for the palliative purpose [15]. However, in the present study, hydroxyurea chemotherapy was performed immediately after incomplete resection of WHO grade II meningioma for the adjuvant purpose.
Surgical resection is usually considered as the best therapeutic option because many meningiomas have benign biologic characteristics. However, the location and anatomical feature of the meningioma is not always suitable for the complete resection. For the WHO grade I benign meningiomas, ‘wait and see’ strategy can be one of options because of the rare recurrence or progression even if the tumor underwent incompletely resection [16]. For the WHO grade III malignant meningiomas, adjuvant radiotherapy is essential even if the tumor was resected completely [9]. Although the necessity of the adjuvant treatment for the WHO grade II meningioma especially in incompletely resected status is usually considered by most neurooncologists, the therapeutic options are still challenging because these tumors are not common enough to be a subject for clinical trials. In the further comprehensive points, there is no report to compare the results of adjuvant radiotherapy versus hydroxyurea chemotherapy for these specific conditions such as incompletely resected atypical meningiomas.
Hydroxyurea, an oral ribonucleotide reductase inhibitor, arrests meningioma cell growth in the S phase of the cell cycle and induces apoptosis [17]. Hydroxyurea chemotherapy in the context of treating patients with meningioma is usually confined to recurrent disease otherwise considered to be inoperable or refractory to radiotherapy, and is considered to be the usual and customary first- and second-line treatments of meningiomas [17]. In a preliminary report by Schrell, hydroxyurea (1,000–1,500 mg/day; 20 mg/kg/day) decreased tumor size in three patients with recurrent WHO grade I meningiomas and prevented recurrence for 24 months in a patient with a completely resected WHO grade II/III meningioma [12]. Several more recent studies suggest that hydroxyurea has modest activity; remissions are uncommon, but some patients appear to have disease stabilization [12131819202122]. In addition, hydroxyurea has been demonstrated to have modest and acceptable toxicity in patients with recurrent meningioma manifested primarily as fatigue and treatment-related anemia. The Southwest Oncology Group (SWOG) conducted the only prospective multi-institution Phase II study to further evaluate the role of hydroxyurea in meningiomas (SWOG-S9811) [21]. This study closed prematurely owing to poor accrual, but preliminary results suggest that hydroxyurea is cytostatic and with moderate hematological toxicity. Problematic with the various hydroxyurea trials, however, is that many patients had not failed to respond to radiotherapy or that radiotherapy was administered concurrently. Although there was the largest retrospective study of hydroxyurea in recurrent WHO grade I meningioma patients, all previously treated with surgery and radiotherapy and in whom no further surgery or radiotherapy was applicable, there were no radiographic responses and 35% of patients had SD [1320212223]. There are several major differences in the present study compared with previous studies; 1) the tumors were confined to WHO grade II meningioma, not included WHO grade I or III meningiomas, 2) the tumors were resected incompletely, 3) hydroxyurea chemotherapy started after surgery as soon as possible without long break, and 4) the patients who underwent hydroxyurea chemotherapy were all radiotherapy-naïve. If there was progression of tumor after adjuvant chemotherapy or radiotherapy, they were essentially considered to be treated with opposite therapeutic modality.
Recently, Champeaux et al. [24] reported the predictive factors for recurrence of atypical meningiomas; the patient's age <57 years at diagnosis, surgical resection in Simpson grade I–III, and Ki67 index <15 were independently associated with longer PFS. Among 178 cases, 7 (3.9%) patients received hydroxyurea chemotherapy and 33 (18.5%) patients underwent the radiotherapy. They reported that radiotherapy as well as hydroxyurea chemotherapy was not associated with PFS in atypical meningiomas. However, they did not use the hydroxyurea for the patient with incompletely resected atypical meningiomas but those with an out-of-control tumor progression; the subjects were also different from our study.
In fact, after the first successful evidence of the hydroxyurea for recurrent and unresectable meningioma was reported, hydroxyurea used to be considered as a standard therapy in the treatment of meningiomas refractory to surgery and radiotherapy in the past. However, sequential studies followed by first successful study have failed to show an anti-tumoral activity in all grades of meningiomas even with tolerable toxicities. Therefore, many medical treatments have been tried and others are under investigation as potential salvage therapy for recurrent or aggressive meningiomas, and include cytotoxic, hormonal and biologic agents. The optimal medical therapies for these subsets of patients are not yet to be determined. Still, several reports are being reported to show the efficacy of hydroxyurea in meningiomas [24].
The unique points of the present study are 1) the comparative results of adjuvant therapeutic modalities with hydroxyurea chemotherapy and radiotherapy was shown 2) in the specific condition of incompletely resected atypical meningiomas. Despite the contributions this study makes to the literature, it has several limitations. First, its main limitation is the inherent bias introduced by its retrospective nature. Indeed, it is difficult to provide sufficient statistical power from such a small number of patients with a recurrence to prove reliable results. We attempted to reduce this bias by collecting patient data from complete medical and radiological records. Before 2011, NCCN guideline for recurrent WHO grade II/III meningioma included the hydroxyurea chemotherapy for recurrent and refractory meningiomas which were surgically inaccessible. However, after 2011, hydroxyurea was excluded but interferon-α, and somatostatin analogue treatments were included in the NCCN guideline. Naturally, before 2011, we tried to treat hydroxyurea for the patients but did not after 2011 according to the NCCN guideline. Therefore, the patients who were treated for atypical meningioma got to be divided into two groups, which we could reduce the selection bias at best. Second, the present study could not reflect the recent trends of medical treatment for recurrent and refractory WHO grade II/III meningiomas. New hormonal therapy including progesterone antagonist and somatostatin analogues, calcium channel antagonist (such as verapamil, nifedipine, and diltiazem), cytotoxic agent (such as temozolomide and irinotecan), and multidrug chemotherapy (such as combination of cyclophosphamide, adriamycin, and vincristine) were not dealt in the present study.
In conclusion, in this retrospective study, we investigated the clinical outcome of the hydroxyurea chemotherapy after incompletely resected WHO grade II atypical meningioma. We also compared the results of hydroxyurea chemotherapy with those of radiotherapy for the adjuvant purpose of reducing the progression. We found that adjuvant treatment after incomplete resection of atypical meningioma are associated with longer PFS than conservative treatment, and that there is no difference of PFS between hydroxyurea chemotherapy and radiotherapy for the incompletely resected atypical meningiomas. Therefore, hydroxyurea chemotherapy can be considered as an adjuvant strategy for the atypical meningiomas if the radiotherapy is impossible. Additionally, surgical extent and proliferative biomarkers such as Ki67, mitosis and p53 are associated independently with PFS.






 XML Download
XML Download