

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chordomas are midline tumors that arise from ectopic cells of notochord remnants, though primarily intrasellar chordomas are uncommon [12]. Although several cases of an intrasellar chordoma mimicking a pituitary adenoma have been reported [13456], a chordoma associated with a pituitary adenoma has been reported in the only 2 cases [78]. Here, the authors report the third case of an intrasellar chordoma with a coincidental pituitary adenoma.
CASE REPORT
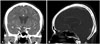
A 68-year-old female presented with slowly progressive diplopia for 1 month when she stared to the right. During the neurological examination, the patient exhibited partial abducens nerve palsy in the right eye, but there was no other neurologic deficit. And, the finding of visual field examination was unremarkable. A computed tomography (CT) scan revealed an intrasellar mass extending to right cavernous sinus. Although the sellar floor was thinned, there was no bony destruction of the skull and no calcification (Fig. 1). Magnetic resonance imaging (MRI) demonstrated a 1.5×2×1.5 cm-sized cystic lesion with a well-enhanced margin and a slightly enhanced inside. The mass compressed the medial wall of the cavernous sinus without invasion (Fig. 2). Pituitary hormone function test revealed normal levels.
Based on the clinical and radiological findings, either a pituitary macroadenoma or a craniopharyngioma were suspected. The patient underwent an endonasal trans-sphenoidal resection. However, an intraoperative finding showed two different tumors in the sella turcica. The first mass was located in the left and anterior side of the sella turcica, and revealed a small and friable tissue with a yellowish color. Whereas, the second cystic mass including a mucoid substance was located in the right side of the sella turcica (Fig. 3). A grossly-total resection was performed.
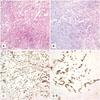
Histopathological findings confirmed two different tumors. First, the yellowish and friable tumor demonstrated as a pituitary adenoma, according to the typical findings of the hematoxylin and eosin (H&E) stain (Fig. 4A). Immunohistochemical stains were negative for prolactin, adrenocorticotropic, and growth hormones. Second, the cystic tumor demonstrated as a chordoma, according to the typical findings of the H&E and immunohistochemical stains (cytokeratin-20 and epithelial membrane antigen) (Fig. 4B, C, and D). Therefore, the present case suggested a coincidental chordoma and pituitary adenoma.
Immediately postoperative MRI demonstrated complete tumor removal. After surgery, the diplopia disappeared, and she did not complain of any symptoms. Pituitary hormone function test also revealed normal levels. Additional treatment, including radiosurgery or proton beam radiotherapy for chordoma, was considered.
DISCUSSION
Chordomas are slow-growing malignant bone tumors, and are thought to arise from notochordal cell rests. Their incidence is rare, and they represent approximately 1% of all malignant bone tumors and 0.2% of intracranial tumors [1]. Their location is usually related to the midline, and approximately 50% develop in the sacrococcygeal region, while 35% develop in the sphenooccipital region and 15% in vertebrae [9].
Most chordomas involving the sellar region likely originate from parasellar or suprasellar bones [2]. Although the incidence of intrasellar chordoma is extremely rare, several studies to date have reported intrasellar chordomas, such as chordomas mimicking pituitary adenomas [13456]. In addition, a chordoma associated with a pituitary adenoma has been twice reported [78]. The first case was a parasellar chordoma combined with a non-functioning pituitary adenoma, and the second case was a clival chordoma associated with a prolactinoma. Therefore, the present case may be the third case of an intrasellar chordoma associated with a coincidental pituitary adenoma.
Radiologically, chordomas are characterized by a solid type, and appear hyperintense on T2-weighted MRI. And, a CT scan may show a destructive and lytic lesion [27]. However, several researchers have reported chordomas during their early development stage and intrasellar chordomas unassociated with sphenoid bone involvement [367]. Similarly, the present case revealed an intrasellar chordoma without sphenoid bone involvement.
In conclusion, we report the third case of an intrasellar chordoma with a pituitary adenoma. Although it may be difficult to distinguish a cystic chordoma without bone involvement from other intrasellar tumors, such as a pituitary adenoma, a craniopharyngioma, or a Rathke's cleft cyst, the present case illustrates that the co-occurrence of two tumors in the sellar region is possible.


 XML Download
XML Download