

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hemangiopericytomas (HPCs) are rare, and are aggressive neoplasms that most often involve the musculoskeletal system and skin [1]. Their occurrence within the cerebellopontine angle (CPA) is exceptional [23456789], but given the considerable overlap of clinical, radiological and pathological features between meningiomas, solitary fibrous tumors (SFTs) and HPCs, and the very aggressive behavior of HPC compared to its counterparts; the differentiation becomes of the utmost importance.
We describe herein an unusual case of a CPA HPC presenting as a right Millard-Gubler syndrome that recurred ten years after radical surgery plus radiation therapy.
CASE REPORT
The patient was a 42-year-old male who presented in June 2004 with complaints of vertigo and dysequilibrium while walking that evolved for four months. He also complained of a slowly aggravating right facial weakness for 3 months associated with ipsilateral facial numbness.
On admission, his neurological examination revealed a right peripheral facial palsy, right abducens palsy, and left hemiparesis, suggesting the presence of the Millard-Gubler syndrome.
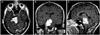
Head CT scan and an MRI of the brain demonstrated a homogeneously enhancing 2.8×3.5 cm sized right CPA lesion causing major brain stem compression without extension into the ipsilateral internal acoustic meatus (Fig. 1).
As the tumor seemed to be dura based, the preoperative diagnosis of a meningioma of the CPA was considered, even though neither dural tail sign nor hyperostosis was observed.
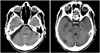
A suboccipital retrosigmoid approach was attempted. During surgery, the tumor was prone to bleeding, and which arose between the Vth and the VII/VIIIth nerve complex with a clear dural basement and no connection with the cranial nerves. There was no tumor within the internal auditory meatus, and although it was fleshy and non suckable, it yielded to cavitron ultrasonic surgical aspirator. Somatosensory evoked potentials, brainstem auditory evoked responses, and intraoperative facial nerve monitoring were used to ensure the safe separation of tumor from the brainstem and associated cranial nerves. Simpson grade II excision was achieved and confirmed on post-operative CT scan (Fig. 2).
The patient recovered quickly with no facial nerve paresis, and was discharged home on the 4th post-operative day.
The histopathology sections revealed a richly vascular tumor with multiple foci of cells with distinct and indistinct cell borders interspersed with small arborizing capillaries. Large irregular blood vessels (staghorn like) were also noticed. The nuclei were round to oval with minimal atypia and few mitotic figures. No necrosis could be observed. Mitotic activity was low but the Ki-67 labeling index was 7%. The cells expressed positivity for vimentin staining and were negative for epithelial membrane antigen. CD34 expression was strongly positive. The morphological and immunohistochemical features strongly favored the diagnosis of a grade II HPC (Fig. 3, Fig. 4).
Metastatic workup including CT of the chest/abdomen/pelvis did not reveal any evidence of extracranial HPC. Adjunctive radiation therapy was administered and a close clinical and radiological follow-up established. He was lost to follow up since March 2008.
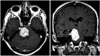
Six years later, the patient was re-admitted to our department with headache and vomiting. At the time of admission, his physical examination revealed a left hemiparesis, and control MRI of the brain showed local recurrence (Fig. 5). The patient refused any secondary intervention and no adjunctive treatment was administered. He died three months later.
DISCUSSION
HPCs are rare, and are aggressive neoplasms that arise from the pericytes of Zimmerman, which are contractile spindle cells surrounding capillaries and post capillary venules [4]; and most often involve the musculoskeletal system and skin [1].
Intracranial HPCs represent only 0.4% of all intracranial tumors [10] and approximately 2% to 4% of all meningeal tumors [5].
Unlike meningiomas, HPCs tend to occur more often in males, with a male-female ratio approaching 2:1 and a mean age of presentation in the fifth decade [11]. The extreme rarity of HPCs at CPA, however, precludes any demographic markers such as age or sex predilection (Table 1).
Since HPCs are difficult to differentiate radiographically from other skull base tumors such as meningiomas, SFTs, and schwannomas; some authors such as Salunke et al. [8] insist on the importance of preoperative planning in suspicious cases of CPA dura based masses and lesions showing disproportionate perilesional edema, narrow base of attachment, or multilobulated cross-leaf growth [12]. Other authors have proposed subtle imaging characteristics that may help to distinguish HPCs from meningiomas, such as the absence of calcification or bony hyperostosis, or the comparison of the apparent diffusion coefficient values in peritumoral edema [813]. Recently, positron emission tomography has emerged as a potentially useful diagnostic tool for differentiating HPCs from meningiomas, but its high cost and availability do not permit routine use in the initial radiological investigation of CPA dura-based lesions. Consequently, the most reliable tool in HPC diagnosis remains as accurate immunohistochemical workup, and although psammoma body and nuclear pseudo inclusions can be found in meningiomas, epithelial membrane antigen negativity and CD34/CD99 positivity assists in the differentiation [5].
Another standpoint is excluding HPC from fibrous variants of SFT (conventional SFT), which have been commonly described to occur at the CPA [14]. Lately, these two entities (SFT and HPC) were believed to represent two parts of the spectrum with fibrous SFT at one end and cellular SFT at the other end. The current World Health Organization classification also acknowledges the overlap, and states these two entities as part of the spectrum [15]. The cellular variant of SFT has lately been proposed to be synonymous with HPC due to considerable morphological and immunohistochemical overlapping [7]. Immunoreactivity for CD34 which is strongly expressed in SFT alone cannot be taken as its diagnostic marker, as 40% of HPC also show reactivity with CD34 [7], and the subunit A of factor XIII once documented as a diagnostic marker for HPC is focally positive in SFT [27]. Therefore, careful histopathological examination is helpful in distinguishing the fibrous variants of SFT from HPC. SFT shows wavy fascicles of elongated undulating cells associated with collagenous bands, whereas HPC shows closely packed, randomly oriented cells with little fibrosis with staghorn sinusoidal vessels and fine reticulin pattern. The neoplastic cells in HPC are also closely packed with little intervening fibrosis.
In the present case, the morphological features were distinctive enough to place the lesion in the category of an HPC. Fairly uniform cellularity of the tumor and the low mitotic activity was more supportive of this lesion being labeled as grade II HPC instead of a cellular SFT.
Unfortunately, the similarities between meningiomas and HPCs end at their radiographic and gross characteristics, as the typical indolent behavior exhibited by most low-grade meningiomas is in stark contrast with the aggressive behavior observed in most cases of HPC. In fact, with a mean survival of 84 months from the time of initial diagnosis [5], a local recurrence rate as high as 91% and a 15-year risk of distant metastasis approaching 70%; intracranial HPCs harbor one of the most aggressive biological/clinical behaviors [16].
Their management relies consequently on a close cooperation between clinicians, surgeons, and pathologists from establishing diagnosis to organizing the therapeutic strategy.
In the current state of knowledge, radical surgical resection, whenever feasible, followed by radiation therapy can be considered as the optimal management policy. Radiation therapy has in fact extended the mean time of local recurrence from 34 to 75 months, and the survival from 62 to 92 months [1].
Depending on the tumor size, some authors advocate the preoperative use of stereotactic radiotherapy as it is associated with the best disease free survival [5], while some others such as Kumar et al. [1], support its role in recurrent disease or re-irradiation. Cho et al. [6] in 2011 reported a case of recurrent CPA HPC 5 years after stereotactic radiosurgery, and supported the use of stereotactic radiosurgery alone for small tumors with the understanding that the tumor may eventually recur. The ten year survival observed here for the first time supports our preferential aggressive surgical approach combined with radiation therapy. Consequently, although we cannot deny the benefits of the use of stereotactic radiosurgery, we do not support its role as the sole therapeutic option in the initial management of these rare and aggressive tumors.
Chamberlain and Glantz [17] in 2008, reported that a chemotherapy protocol combining: cyclophosphamide+adriamycin+vincristine, followed by α-interferon, followed by ifosamide-carboplatin-etoposide, may be helpful for recurrent intractable cases, but such encouraging results was tempered by other studies that observed no real place for chemotherapy in the available therapeutic armamentarium of intracranial HPCs.
In the present case, no chemotherapy was administered either in the initial management or at recurrence.
In conclusion, given the clearly aggressive nature of intracranial HPCs, it becomes imperative to include them in the differential diagnosis of CPA dura based tumors.
A high index of suspicion on radiology imaging is essential to plan for total excision, and an accurate histopathological diagnostic precision is of the utmost importance.
As postoperative recurrence seems unavoidable, long-term follow-up with serial imaging should be considered in all cases.



 XML Download
XML Download