

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Schwannomas are predominantly benign nerve sheath tumors composed of Schwann cells; the tumors can grow anywhere throughout the nervous system that contains Schwann cells [1]. The most common place for intracranial schwannomas is the posterior fossa of the brain. Intracranial schwannomas account for 6-8% of all intracranial tumors [2]. Most commonly, schwannomas arise from the 8th cranial nerve, and less frequently from the 5th, 9th, 10th, and 7th cranial nerves. The occurrence of a schwannoma not related to the cranial nerves is extremely rare [2]. Because the olfactory and optic nerves lack a Schwann cell layer, these are not prone to develop into a schwannoma [3,4]. We present an unusual case of an olfactory groove schwannoma along with brief review of the literature.
CASE REPORT
Clinical features and radiology findings
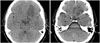
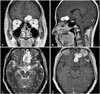
A 49-year-old woman presented with headache, nausea, and vomiting for a few days. Her neurological examination was unremarkable, and she denied any symptoms of olfactory dysfunction. Computed tomography displayed an abnormal low density in the left frontal lobe (Fig. 1). T1-weighted magnetic resonance imaging (MRI) revealed a hypo-intense mass lesion in the left frontal base and displacement of the right frontal base contralaterally. T2-weighted MRI demonstrated an interspersed high signal intensity in the mass, implying the presence of a cystic component. Further MRI with gadolinium enhancement showed a 3 cm sized variegating enhanced mass attached to the cribriform plate (Fig. 2).
Operation and progress
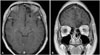
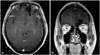
The patient underwent complete resection via the subfrontal approach. During the operation, the tumor was yellowish and well demarcated, but strongly attached to the cribriform plate. The pathologic diagnosis was a schwannoma. Histopathology revealed a typical schwannoma composed of spindle cells and Verocay bodies (Fig. 3). Postoperatively, her headache improved and her olfaction was also preserved, and the patient was discharged without neurologic deficits (Fig. 4). Follow-up MRI at 19 months showed no evidence of tumor recurrence (Fig. 5).
DISCUSSION
Schwannomas arise from Schwann cells of the nerve sheath. It is bewildering that schwannomas can arise from the olfactory nerve, which lacks a Schwann cell layer. However, some hypotheses about the genesis of olfactory groove schwannoma are centered on its developmental and non-developmental origins [5,6]. The developmental hypotheses suggest whether mesenchymal pial cells to transform into ectodermal Schwann cells or neural crest cells to migrate within the substance of the central nervous system [5,6]. The non-developmental hypotheses postulate that intracranial schwannomas arise from the Schwann cells normally presenting in the adjacent structures, such as the perivascular nerve plexus, the meningeal branches of the trigeminal and anterior ethmoidal nerves innervating the anterior cranial fossa and olfactory groove [5,6]. In most cases, cystic degeneration and lipid accumulation wrapped in a collagenous capsule can be found. Schwannomas react strongly to S-100 protein in immunohistochemistry [5]. Li et al. [6] gathered previous literatures and reported that results in 35 cases of olfactory schwannomas (between 1974 and 2010) has shown that 14 out of 30 cases (47%) (with the exclusion of five cases due to unknown olfactory function) had preserved olfactory function, but that the remaining 16 (53%) experienced either anosmia or hyposmia. Regarding the attachment sites of the schwannomas, they sum-marized that 12 cases were on the cribriform plate, 10 cases were on the olfactory groove, and 5 cases were on the skull base and skull base dura. When the tumor was attached to the cribriform plate, the rate of olfaction preservation was relatively high [9 of 11 cases (82%), excluding one case due to unknown olfactory function], compared to olfactory groove attachment [2 of 7 cases (29%), excluding three cases due to unknown olfactory function]. In our case, the tumor was attached to the cribriform plate, and we achieved gross total resection without compromising her olfactory function.
Because most olfactory region schwannomas have a benign nature, a complete resection of the tumor is the treatment of choice, and adjunctive therapy is not usually required [1,3]. In addition, its prognosis after complete resection is known to be favorable [3].
In conclusion, schwannomas of the olfactory groove are extremely rare. When the tumor is attached to the cribriform plate, the preservation rate of olfactory function is higher compared to nearby structures. We reaffirmed that complete surgical resection is a curative modality. In the case of anterior cranial fossa tumor, a schwannoma should not be overlooked in the differential diagnosis.

 XML Download
XML Download