

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Glioblastoma is the most common malignant primary brain tumor and has a rapid progressive clinical course and then fatal outcome [1,2,3,4,5]. The standard therapy for glioblastoma is a surgical resection followed by concurrent chemoradiotherapy (CCRT) using temozolomide (TMZ) [6]. Despite standard therapy for glioblastoma, the median overall survival (OS) is only 14.6 months [6,7].
According to the literature, about 50% of cases occur in patients aged 65 years or older [1,2,4]. However, the trial by Stupp et al. [7] included only younger patients for standard therapy and several other important clinical trials also excluded elderly patients due to poor outcomes in this group, which could be related to age-dependent underlying molecular differences [1,4,8].
In elderly patients, standard therapy for glioblastoma may bring about additional side effects. While the ratio of elderly patients is steadily increasing, there is a necessity to analyze the outcome of the effect of standard treatment in elderly patients with glioblastoma. Thus, in this study, we analyzed the outcome of the treatment of elderly patients with glioblastoma and compared it with that of younger patients.
Go to : 
MATERIALS AND METHODS
Patient population
This study was approved by the Institutional Review Board of the authors' hospital. The author's hospital database was used to identify patients with histologically confirmed glioblastoma between January 2006 and December 2013. Seventy-five patients were diagnosed as glioblastoma pathologically. Eleven patients with secondary glioblastoma were excluded because they had a previous chemotherapy or radiotherapy history. Therefore, 64 patients were selected for this study. We regarded the 'elderly patient' as aged 65 years or over according to the traditional concept, government law concering elderly patient care and geriatric medicine. The elderly group included 16 patients who were aged 65 years or over at the time of histopathologic diagnosis. The control group included 48 patients who were younger than 65 years. Data was collected by using chart review, surgical reports, and brain magnetic resonance imaging (MRI).
Characteristics of patients
Table 1 shows the characteristics of patients. The median follow-up period of the patients who were included in this study was 12 months (range, 2.1-78.2 months). There were 37 men and 27 women, with a median age of 54 years (range, 10-82 years). In the control group, there were 26 men and 22 women, and the median age of this group was 50 years (range, 10-64 years). In the elderly group, 11 men and 5 women were included and the median age of this group was 71 years (range, 65-82 years).
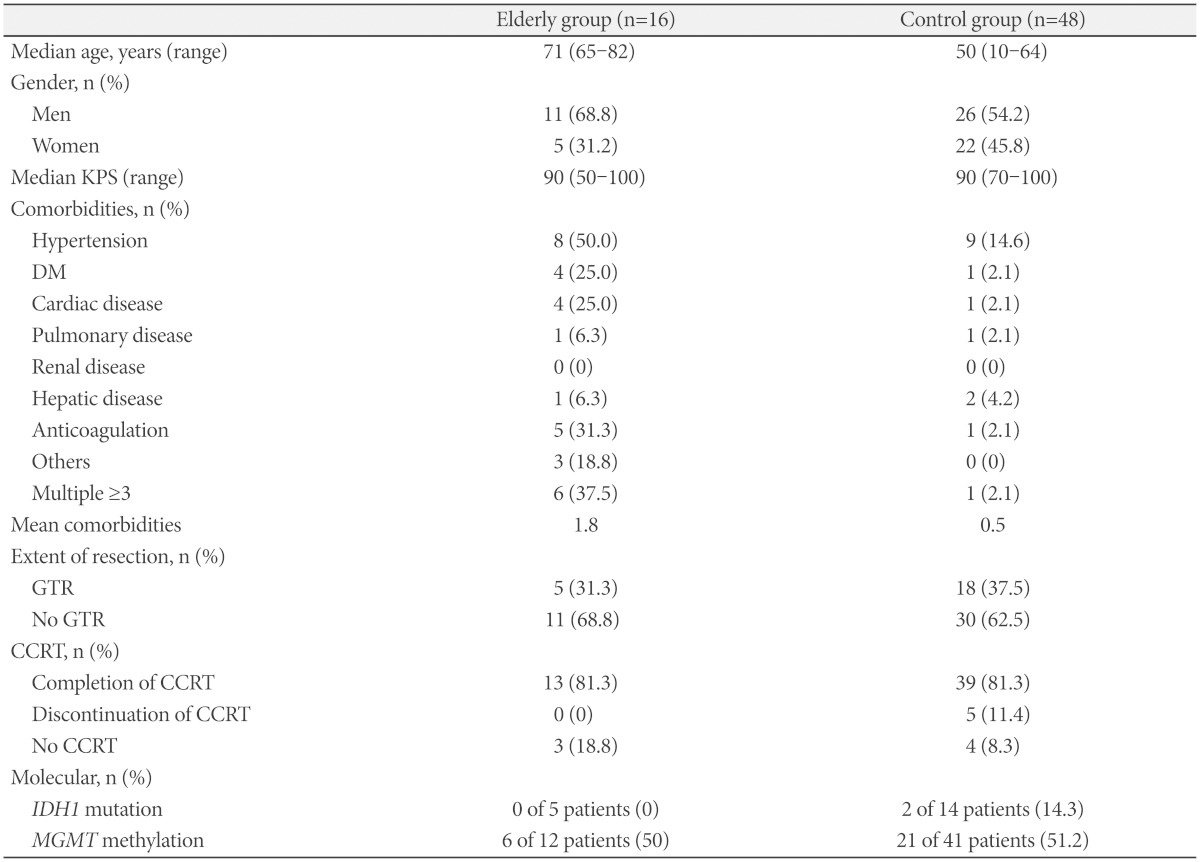
The median Karnofsky Performance Scale (KPS) was 90 and there was no difference between the two groups. The KPS range was from 50 to 100 in elderly group and 70 to 100 in the control group.
We investigated pre-existing medical comorbidities including hypertension, diabetes mellitus (DM), cardiac disease, pulmonary disease, renal disease, hepatic disease, use of anticoagulation, and others. The most common comorbidity was hypertension in both groups. The next common comorbidity in the elderly group was DM (25.0%) and cardiac disease (25.0%), while it was hepatic disease (4.2%) in the control group. Six patients (37.5%) had 3 or more pre-existing comorbidities in the elderly group while there was just one patient (2.1%) in the control group. Mean number of medical comorbidities was 1.8 in the elderly group and 0.5 in the control group.
Patients underwent either open resection or stereotactic biopsy for diagnostic purposes. The extent of resection was assessed by the patients' postoperative brain MRIs taken within 48 hours after surgery. The resection extent was classified into 3 groups: "grossly total resection (GTR)", "partial resection (PR)", and "biopsy". GTR was defined as no residual enhancing lesion, and PR as residual enhancing lesion after open resection. Patients who underwent stereotactic biopsy were included in the biopsy group. GTR of tumor was achieved in 23 patients (35.9%) for all patients; 5 patients (31.3%) belonged to the elderly group and 18 patients (37.5%) to the control group. The patients with PR were 39 of 64 patients (60.9%), and only a biopsy was performed in 2 of 64 patients (3.1%).
Radiotherapy regimens were 2 Gy given 5 days per week for 6 weeks, for a total of 60 Gy and chemotherapy regimens were continuous daily temozolomide (75 mg per square meter of body surface area per day, 7 days per week from the first to the last day of radiotherapy). Fifty-two of 64 patients (81.3%) had completed CCRT, and among them, 13 patients (81.3%) belonged to the elderly group and 39 patients (81.3%) to the control group. Five patients (11.4%) discontinued CCRT and they were all in the control group. Seven of 64 patients (10.9%) could not start the CCRT after surgery, and among them, 3 patients (18.8%) belonged to the elderly group and 4 patients (8.3%) to the control group.
Nineteen patients were investigated for isocitrate dehydrogenase 1 (IDH1) mutation. IDH1 mutation was positive in none of 5 patients of the elderly group and 2 of 14 patients (14.3%) of the control group. Fifty-three patients were also investigated for O6-methylguanine-DNA methyltransferase (MGMT) status (methylated vs. unmethylated); 6 of 12 patients (50.0%) in the elderly group and 21 of 41 patients (51.2%) in the control group had methylated MGMT.
Statistical analysis
All analyses were done with Version 21.0 of IBM SPSS (SPSS Inc., Chicago, IL, USA). The log-rank test was used to get progression free survival (PFS) and OS. PFS was defined as the time interval between initial diagnosis and recurrence or progression on brain MRI, and OS was calculated from the time of initial diagnosis to that of death by any cause. Multivariate analyses of risk factors were performed using the Cox proportional hazards model. The following variables were analyzed for correlation with clinico-oncologic outcome: age, extent of resection, status of CCRT, MGMT methylation status, and combined disease status including hypertension, diabetes insipidus, pulmonary disorder, heart disorder, renal disorder, hepatic disorder, use of anticoagulation treatment and others.
Go to :
RESULTS
Overall outcome
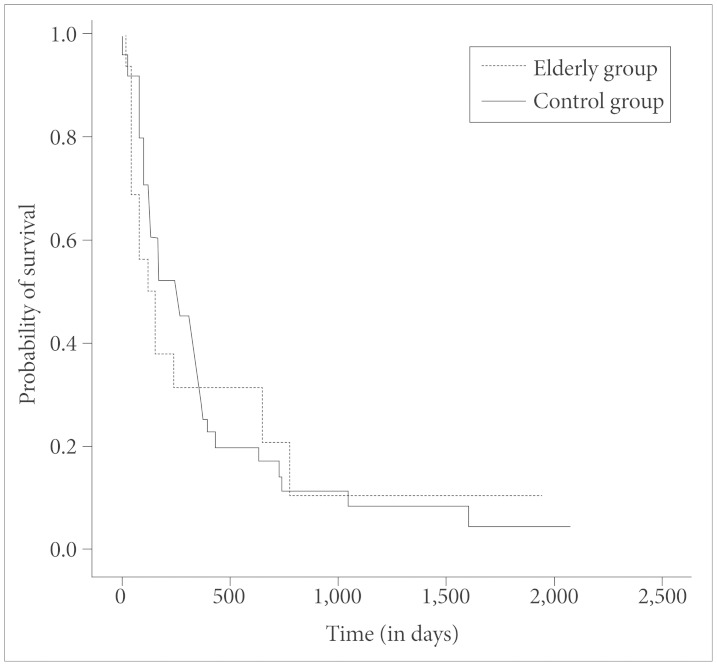
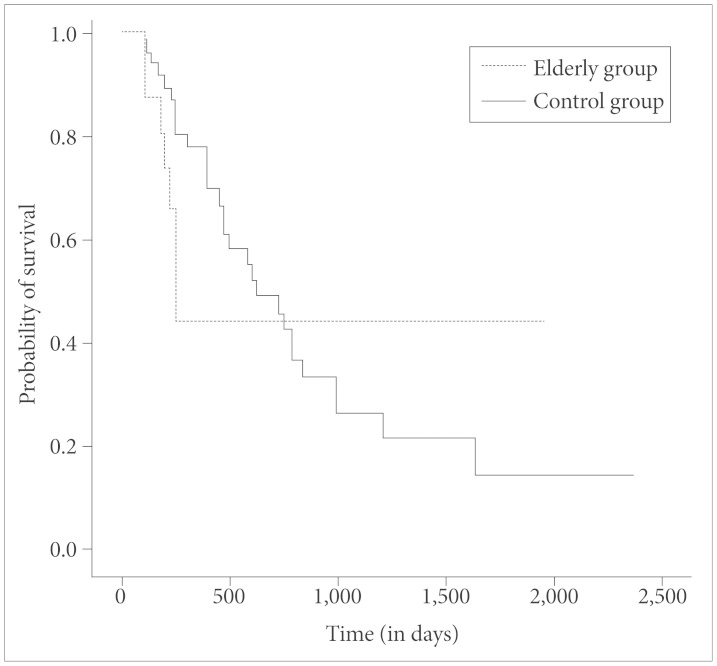
At the time of this study, 37 of 64 patients had expired. The median PFS was 5.6 months and the median OS was 19.9 months in all patients. The median PFS was 8 months in the control group vs. 4.2 months in the elderly group (Fig. 1), but there was no statistical significance (p=0.762). The median OS was 20.9 months in the control group vs. 8.2 months in the elderly group (Fig. 2), but there was also no statistical significance (p=0.457).
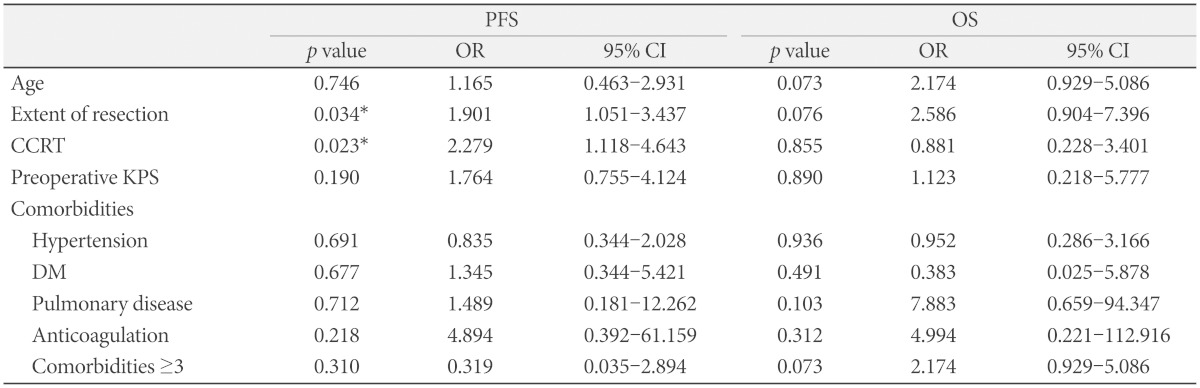
Prognostic factors for survival
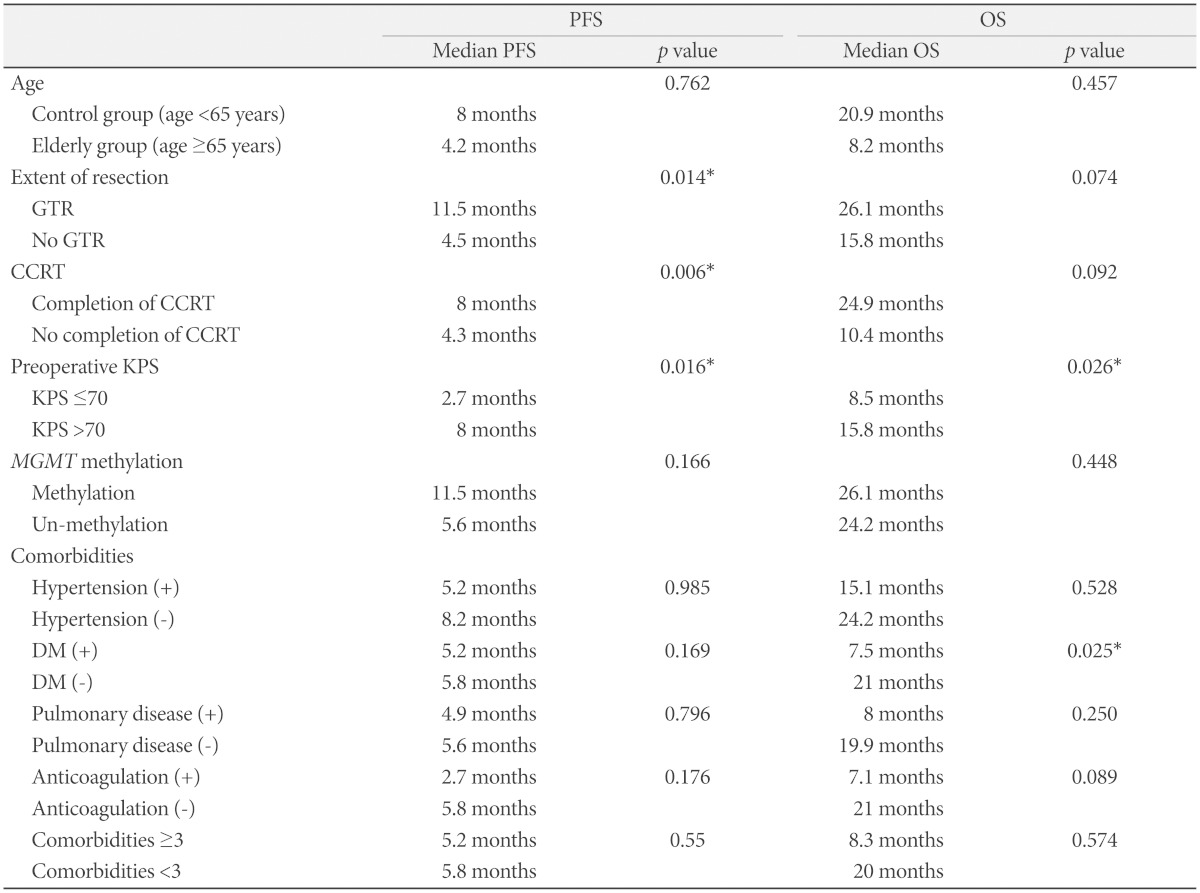
Table 2 shows the outcome of this study including prognostic factors in univariate analysis. In univariate analysis, prognostic factor for PFS with a statistical significance were extent of resection, completion of CCRT, and preoperative KPS, and for OS were preoperative KPS and presence of DM. Multivariate analysis of factors associated with PFS and OS was done except for MGMT methylation and IDH1 mutation due to the difference in the number of patients tested for the two factors. Table 3 shows the results of multivariate analysis. Extent of resection and completion of CCRT were identified as independent prognostic factors for PFS. There was no independent prognostic factor for OS in multivariate analysis. In this study, age was not a prognostic factor for PFS and OS in both univariate and multivariate analyses.
Tolerability to surgery
For all patients, systemic postoperative complications occurred in six patients. Among them, two patients were belonged to the elderly group. One of 2 patients who was 78 years old needed intensive care unit (ICU) care for nine days due to pulmonary congestion, pneumonia and acute renal failure. Other patients who belonged to the elderly group had no need for extension of ICU stays for medical reasons.
Mean duration from surgery to CCRT was 17.7 days in the control group and 16.3 days in the elderly group. The postoperative recovery period did not show a significant difference between the two groups.
Postoperative intracranial hemorrhage occurred in three patients (3 of 64 patients, 4.7%). Among them, one patient (1 of 46 patients, 2%) was in the control group and two patients (2 of 16 patients, 12.5%) in the elderly group. Cerebral infarction was found in one patient who was in the elderly group and status epilepticus was also observed in one patient who belonged to the elderly group.
Tolerability to concurrent chemoradiotherapy
Fifty-two of 64 patients (81.3%) completed postoperative adjuvant CCRT and there were no differences between the two groups. In the control group, 44 of 48 patients (91.7%) started CCRT after surgery and 5 of 44 patients (11.4%) could not complete CCRT. Therefore, 39 of 48 patients (81.3%) completed CCRT in the control group. In the elderly group, 13 of 16 patients (81.3%) started CCRT after surgery, and they all finished CCRT.
Disease progression rapidly occurred in 4 patients and one patient discontinued CCRT due to a severe skin rash. On the other hand, in the elderly group, 13 of 16 patients (81.3%) started CCRT and all of them finished CCRT.
Reported side effects in the patients who were finished CCRT showed that 13 of 52 patients (25%) suffered from minor gastrointestinal problems and 7 of 52 patients (13.5%) from alopecia. Two of 52 patients (3.8%) were observed to have leukocytosis. Skin rash occurred in 2 of 52 patients (3.8%).
Go to :
DISCUSSION
The significance of brain tumor treatment in elderly patients has been emphasized due to the progressive increase in life expectancy [9]. As a result of the significant increase in the incidence of glioblastoma in the elderly [10,11], treatment of glioblastoma in this group is becoming more important [8,9]. About half of patients with glioblastoma are older than 65 years in most western countries [1,12], and its incidence in elderly patients will continue to increase because the elderly group of the population is growing faster than other groups [13]. The incidence of glioblastoma in patients aged over 65 years has doubled from 5.1 per 100,000 in the 1970s up to 10.6 per 100,000 in the 1990s in Los Angeles County [14,15]. Now, the median age of patients with glioblastoma is about 65 years [14].
Although there are standard therapies for glioblastoma such as a surgical resection followed by CCRT using TMZ [6,16], the natural history of glioblastoma is to take a rapidly progressive clinical course, followed by a fatal outcome [1,2,3,4,5,12]. Actually, despite standard therapy for glioblastoma, the median OS for glioblastoma is only 14.6 months [6,7,14,17]. Elderly patients have a poorer prognosis than younger patients and median survival is only 4-5 months in these patients [14,16]. Reasons for poorer prognosis in elderly patients may include 1) less favorable molecular signatures; 2) receipt of less care including surgery, radiation therapy (RT), and chemotherapy; and 3) treatment toxicity and comorbidities as compared with younger patients [14].
The trial by Stupp et al. [7] included only younger patients for standard therapy and several other important clinical trials also excluded elderly patients due to poor outcomes in this group [1,4,8,13,14]. In population-based reviews of the management of elderly patients with glioblastoma, a large proportion of these patients did not receive the standard therapy [12,18]. Kita et al. [19] reported that the proportion of glioblastoma patients who were treated with only supportive care increased with age. And Barnholtz-Sloan et al. [20] also reported that multidisciplinary therapy was less common in elderly patients. Actually, standard therapy for elderly glioblastoma patients does not exist [10,13,14,21]. This means great variability in treatment for elderly glioblastoma patients in many countries and centers [13].
In this study, we applied the standard therapy for glioblastoma to an elderly group and control group. Thanks to the recent improvements made in neurosurgery [9], surgery for glioblastoma was tolerable for elderly patients in this study. There were a few complications after surgery. Postoperative intracranial hemorrhage occurred in three patients (4.7%) and among them, two patients in the elderly group. Cerebral infarction was found in one patient in the elderly group, and one patient in the elderly group was diagnosed with status epilepticus after surgery. Tolerability in CCRT was also shown for both groups. Fifty two of 64 patients (81.3%) were treated with CCRT and the results were the same between both groups. The side effects of CCRT were minimal. Only one patient in the control group discontinued CCRT due to a severe skin rash.
Although our study's patient number could be considered small, the results of this study suggests that the standard therapy for glioblastoma provides a tolerable clinical and oncological outcome for patients who are aged 65 years or over with primary glioblastoma. Elderly patients often believe that they need longer to recover from aggressive neurosurgery and have a high risk for surgical complication [2,22]. However, this study shows that elderly patients are also tolerable to aggressive tumor resection as is the control group. Oszvald et al. [23] who reported on elderly glioblastoma patients and matched the patients to their younger counterparts confirmed that elderly patients may benefit from aggressive surgery. An increased risk of CCRT toxicity with age was generally known [14,16,21,24], but other studies also show acceptability to RT with TMZ chemotherapy [10,25]. In this study, elderly patients could tolerate treatment of CCRT as younger patients. Minimal side effects were tolerable in almost all patients including the elderly.
According to previous studies, prognostic factors for elderly patients with glioblastoma are preoperative KPS, extent of tumor resection, radiotherapy, chemotherapy, and MGMT methylation status [6,7,8,26]. Our study identified the extent of tumor resection, completion of CCRT, and preoperative KPS as independent prognostic factors in univariate analysis, and extent of resection and completion of CCRT in multivariate analysis. However, age and MGMT methylation status were not a prognostic factor.
This study has several limitations. It is retrospective and uses a small sample size. Unusual high proportion of positive MGMT methylation status was found in this study. This can be presumed to be the reason why the MGMT methylation status is not a prognostic factor. According to molecular studies in glioblastoma, there are substantial differences in important features at the methylation status of the MGMT promoter [27]. All except for one Russian patient are Koreans, and there is a difference in ethnic group compared to other studies. IDH1 mutation is not considered to be significant due to a small number of patients.
Nevertheless, our study may be meaningful and support the finding that elderly glioblastoma patients could be treated by standard therapy and future prospective clinical studies will be needed to establish a standard of treatment for elderly glioblastoma patients.
In conclusions, surgical resection and CCRT were well tolerated in elderly patients with glioblastoma. Clinical and oncologic outcome were not affected by age or medical comorbidities. In elderly patients, maximal safe resection followed by timely CCRT could improve clinico-oncologic outcomes.
Go to :
 XML Download
XML Download