

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Current treatment strategies for benign perioptic tumors include observation, surgical resection, and irradiation techniques [1,2,3,4]. Complete surgical resection is the ideal treatment in most cases, but, even with modern neurosurgical techniques, is sometimes not possible without significant morbidity or mortality. Radiation therapy (RT) or stereotactic radiosurgery (SRS) can be considered for residual or recurrent lesions after surgery or can be used as a primary treatment modality when patients cannot undergo surgery [5,6]. SRS is preferred for small lesions and is usually performed in a single session. An excellent tumor control rate has been reported for many intracranial tumors treated by radiosurgery [7]. However, the proximity of the anterior visual pathways poses a particular challenge for ablating "perioptic" tumors. It is widely acknowledged that the unique radiation sensitivity of the normal optic apparatus precludes conventional SRS when a lesion is within 2 mm of the anterior visual pathways [1].
Although numerous clinical series of these lesions suggesting optimal dose and fractionated regimens of RT have been published [8,9,10], the tumor control rate is not quite as good as that achieved with SRS [1,5,11]. In addition, an almost 3% risk of optic neuropathy and a 30% to 70% risk of endocrinological dysfunction have been reported [1]. Fractionated radiosurgery can provide a compromise that offers the efficacy of SRS and the safety of fractionated radiotherapy. Recent trials of fractionated CyberKnife radiosurgery for perioptic tumors have demonstrated effective tumor control equal to that of single session radiosurgery, while maintaining a low optic neuropathy risk comparable to that of fractionated RT [1,12]. Gamma Knife has been used almost exclusively for single session radiosurgery, and few formal reports of fractionated Gamma Knife radiosurgery (GKRS) have been published. We previously reported interim acceptable visual results for 22 patients after fractionated GKRS [12]. In this study, we analyzed the outcomes of tumor control and visual preservation for 38 perioptic tumor patients after fractionated GKRS.
Go to : 
MATERIALS AND METHODS
Patient population and clinical assessment
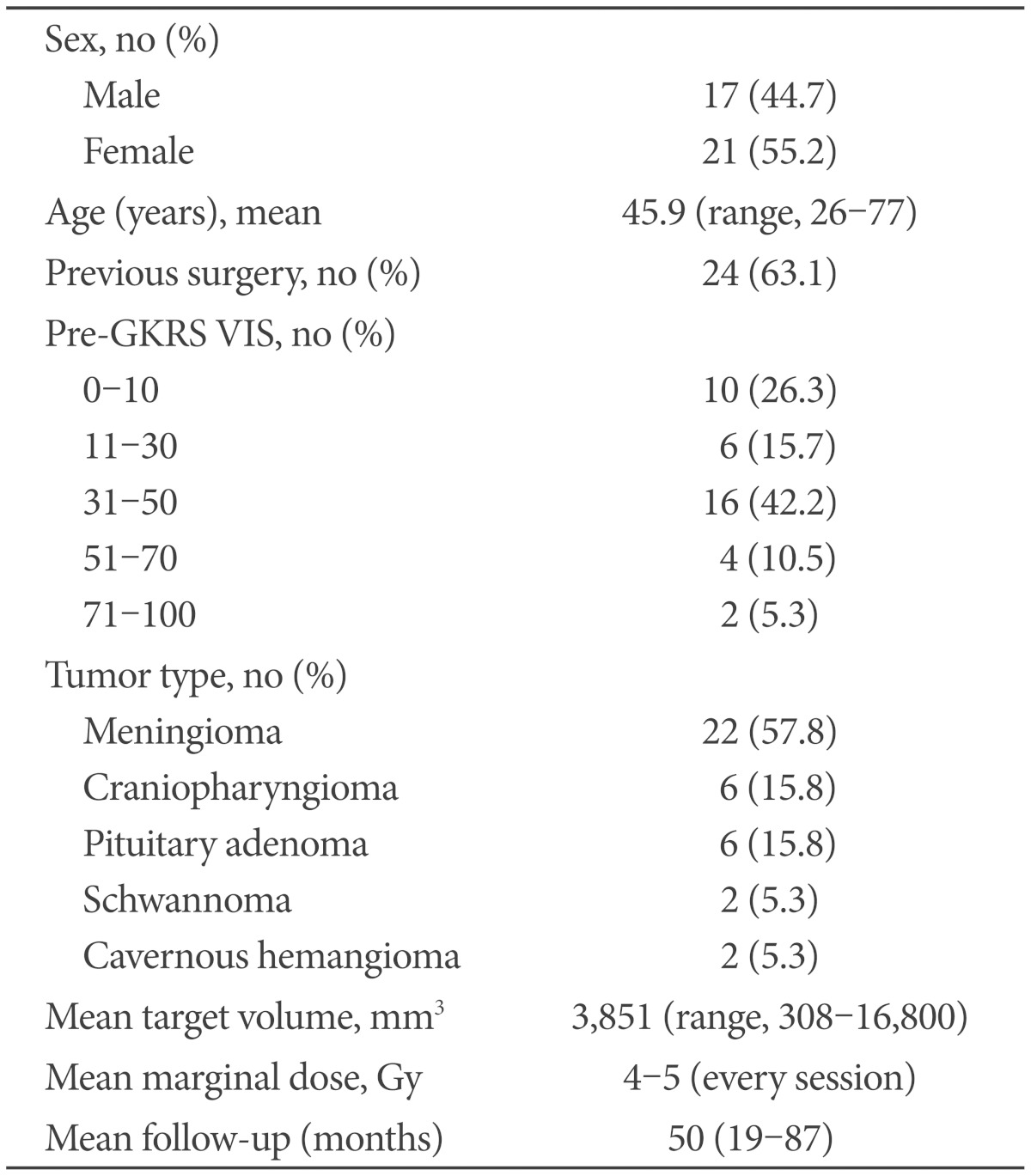
Thirty-eight patients with perioptic tumors were treated with fractionated GKRS at our institute between May 2004 and December 2008. We analyed medical records and radiological data, retrospectively (Table 1). There was no high signal intensity gap between the tumors and the optic pathway on T2-weighted magnetic resonance imaging (MRI) scans in any patients, suggesting direct contact between the structures. Therefore, these patients were not eligible for typical single session GKRS. Among the 38 patients, open surgical resection had been previously performed in 24 patients.
Each patient was evaluated before SRS by thin-slice contrast-enhanced MRI. In assessing tumor control, a greater than 20% increase or decrease in tumor volume post-GKRS compared to pre-GKRS was considered an "Increase" or "Decrease", respectively. Changes less than 20% were considered "Stationary".
Visual acuity and visual fields were analyzed according to the visual impairment score (VIS) using guidelines from the German Ophthalmological Society [13]. Scores ranged from 0 to 100 (worst). Snellen visual acuity was assessed at a 5 m distance. The change in visual acuity was defined as visual acuity change of one or more Snellen lines. Unserviceable visual acuity (score of visual acuity=0) included no perception of light, hand movement, or counting fingers. Any improvement or deterioration among those with unserviceable visual function was not considered functional change. Visual function was assessed pre- and post-GKRS (at least six months after GKRS). The visual outcome results were classified using VIS as "Improved" (lower score), "Stationary" (unchanged), or "Aggravated" (higher score). The "Improved" and "Stationary" groups were classified as "Favorable", while the "Aggravated" rating was considered "Unfavorable". Serum hormone levels were measured in patients with pituitary adenoma. The Institutional Review Board at our institute approved this study (IRB file number: 2011-05-004-001).
SRS technique
Stereotactic radiosurgery was carried out using the Leksell Gamma Knife B and C system (Elekta Instruments AB, Stockholm, Sweden). In all patients, radiation was delivered in four sessions with 12 hours between each session. On the morning of the first day of fractionated GKRS, a Leksell stereotactic frame was applied under local anesthesia. The frame was retained until completion of the last irradiation session. T2-weighted axial images with a slice thickness of 2 mm and three-dimensional spoiled gradient-recalled images with double-dose contrast enhancement were acquired at a slice thickness of 1 mm without a slice interval. The fat suppression technique was used to improve delineation of the optic nerve in patients with intraorbital lesions. Radiosurgery planning was performed using Leksell Gamma plan version 5.34 (Elekta Instruments AB, Stockholm, Sweden). The dose plan was similar to that of typical single session GKRS, except that the prescribed doses were adjusted for fractionated treatment.
We approximated patient skull shape at every procedure session and confirmed that the measurements were unchanged. Further, MRI was performed before GKRS and just before the last session in order to detect possible stereotactic frame displacement and to verify the stable geometric coordinates of definite landmarks including round enhancing structures. The mean discrepancy between the landmark structure coordinates measured in each MRI was 0.19 mm (range, 0-0.56 mm).
The mean target volume was 3,851 mm3 (range, 308-16,800 mm3) and the marginal dose administered per session was 4-5 Gy. Therefore, a median cumulative dose of 20 Gy (range, 16-20 Gy) was prescribed at the tumor margins. The median prescription isodose was 50% (range, 42-55%).
Go to :
RESULTS
The post-GKRS results are summarized in Table 2. The median follow-up period was 38.2 months (range, 6-81 months). MRI follow-up was performed in 37 patients (mean, 32 months). Tumor volume decreased in 12 (31%) patients and had remained stable in 23 (61%) patients at the last follow-up visit. Therefore, tumor growth control was achieved in 35 (94.6%) patients. Tumor volume increased in two craniopharyngioma patients. One patient experienced progressive tumor growth with visual deterioration and underwent surgical resection nine months after fractionated GKRS. Tumor regrowth without visual impairment was observed in another patient 15 months after fractionated GKRS and additional endoscopic resection was performed.
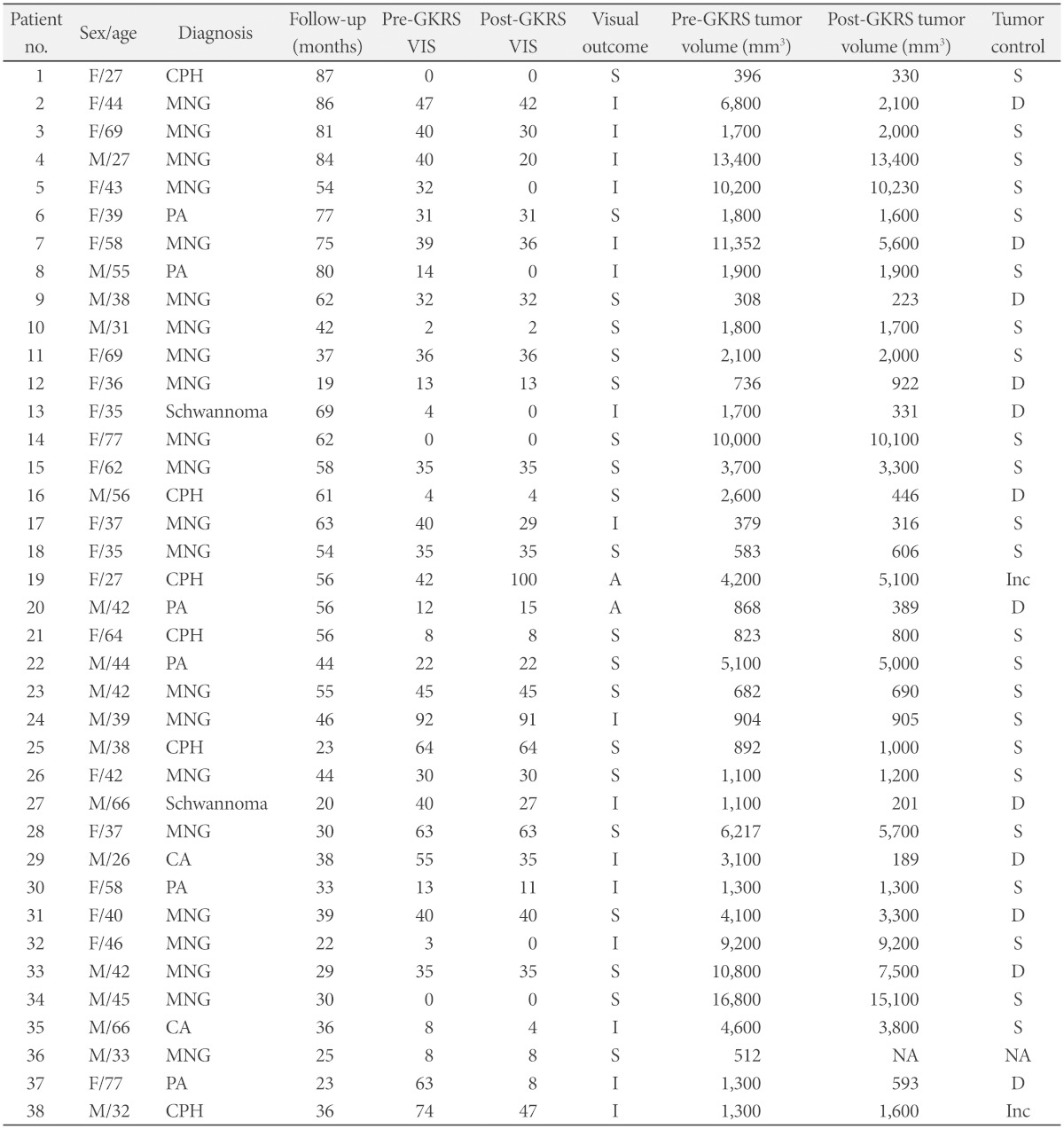
The average VIS was 30.6 in the pre-GKRS periods and 26.3 at the last post-GKRS follow-up (mean, 11 months; range, 6-50 months). Favorable visual outcomes in the postoperative period were achieved in 94.7% of cases (36/38). After GKRS, 16 of the 38 patients had improved visual function. Twenty cases showed stationary VIS at the last follow-up visit, and a craniopharyngioma patient showed deteriorated visual function after GKRS due to tumor progression. Another patient with a pituitary adenoma showed mild (subjectively not deteriorated) deterioration on post-GKRS examination (VIS was decreased three points after GKRS) even though the tumor was controlled after GKRS. Endocrinologically, no patients showed hypopituitarism after fractionated GKRS except for six craniopharyngioma patients.
Two patients with functional pituitary adenoma were recruited in this series. In one patient with McCune-Albright syndrome, growth hormone levels decreased significantly at 23 months after fractionated GKRS with tumor shrinkage, though levels did not normalize. In one prolactinoma patient, the tumor volume was stationary. However, serum prolactin levels were normalized after administration of bromocriptine. No permanent complication or treatment-related morbidity occurred. A representative case with a orbital hemangioma is shown in Fig. 1.
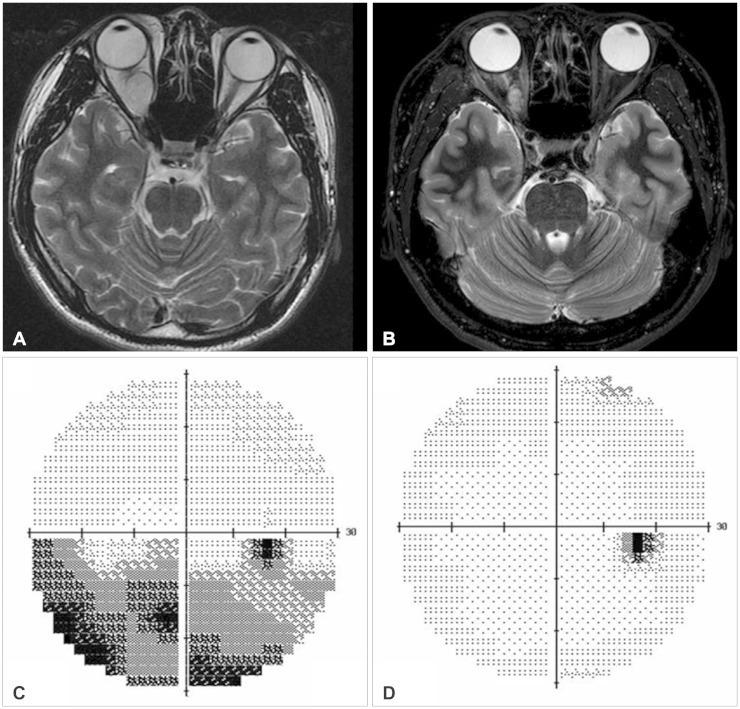 | Fig. 1A 26-year-old male patient (case No. 29) with a right orbital hemangioma underwent fractionated Gamma Knife radiosurgery. A comparison of the magnetic resonance images acquired before radiosurgery (A) and 15 months after radiosurgery (B) reveals a decrease in tumor volume. Visual field examination shows a field defect before radiosurgery (C) and only a small blind spot 12 months after radiosurgery (D).
|
Go to :
DISCUSSION
Tumor control and visual preservation are major concerns for the treatment of perioptic lesions. Surgical optic nerve decompression is the treatment of choice for patients with these lesions. However, in spite of recent advances in imaging modalities and operative techniques, many perioptic tumors are not readily resectable due to critical location and patient factors including old age and poor medical condition. The role of RT in perioptic tumors as primary treatment or adjuvant treatment after resection has been reported by several authors. Long-term local control ranges from 68% to 89% for benign lesions [14,15,16,17] and 53% for craniopharyngioma [18], although RT is safe and effective for those tumors. Irradiation of adjacent structures and optic nerve injury caused by inaccuracy of the treatment fields are major limitations of conventional RT and even fractionated methods [5,10,19]. In addition, a six week course of between 45 and 55 Gy using 1.8 to 2 Gy fractions may be inconvenient for many patients.
Fractionated SRS aims to integrate the advantages of conventional fractionated RT and single-session radiosurgery. Adler et al. [1] suggested that radiation delivered accurately may benefit from the "volume effect" (i.e., irradiation tolerance inversely proportional to the length of the irradiated nerve), which permits larger doses to be delivered per session without increasing the complication rate. Furthermore, a larger dose per fraction results in a higher biological equivalent dose and allows greater tumor control [11]. For perioptic lesions, multi-session GKRS may enable higher rates of tumor control than conventional RT without increasing the risk of optic neuropathy. It also has a shorter treatment period than conventional fractionation RT. For fractionated radiosurgery, CyberKnife would be more convenient for patients than Gamma Knife as it does not require a frame. Nonetheless, the excellent accuracy and conformity of GKRS may facilitate fractionated SRS for those lesions.
In this study, tumor control and preservation of visual function over a mean follow-up period exceeding three years were noted in the majority of patients. Our results are comparable to the 96% tumor control and visual preservation rate of a prior study [1]. Because of the inconvenience of stereotactic frame fixation, GKRS has traditionally been used for single session treatments. However, in this study, fractionated GKRS over three days was tolerated by most patients. Although the discomfort associated with rigid frame fixation is certainly a disadvantage, it minimizes inter-fractional displacement errors, as demonstrated by our data. Therefore, fractionated GKRS can be considered more reliable than procedures without rigid fixation. Furthermore, the higher cumulative energies delivered to targets by GKRS may be another advantage because the marginal dose is prescribed at the 50% isodose line rather than at the larger isodose line used for other systems.
In the selection of dose and number of sessions, we made reference to other reports of empirically derived fractionation using RT or radiosurgery and tried to irradiate with the lowest possible dose to the optic apparatus. Even though we verified the safety and intermediate-term efficacy in a previous pilot study [12], the optimal dose and fractions remain uncertain. Surely, many important variables including pathology, tumor volume, and history of previous RT or surgery should be considered. Further long-term prospective studies with a larger numbers of patients, and comparisons between fractionated GKRS and standard fractionated RT and low-dose single session SRS are required to confirm the validity of the procedure. Despite the remaining uncertainties, we suggest that fractionated GKRS should be considered as a safe tool for increasing the probability of tumor control and preserving visual function for perioptic tumor intervention.
Go to :
 XML Download
XML Download