

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intracranial dermoid cysts are rare congenital lesions that have been reported to account for 0.04 to 0.7 percent of all intracranial tumors [1]. Intracranial dermoid cysts occur at the midline strand, and two thirds of these tumors are found at the posterior fossa [2,3]. Dermoid cysts are commonly located at intradural portions of the parasellar and midline frontobasal regions [1]; however, they are rarely found in the extradural location. In the present study, we report an intracranial extradural dermoid cyst at the lateral sphenoid ridge accompanied by bone erosion.
Go to : 
CASE REPORT
History and examination
A 53-year-old woman was admitted because of progressive headache, nausea, and dizziness lasting one month. On neurological examinations, no deficit was detected. On computed tomography (CT) scan, a low attenuating lobulated mass was observed at the right sphenoid ridge, and the lesion was accompanied by bone erosion. There was no extracranial communication with the scalp (Fig. 1). Magnetic resonance imaging (MRI) of the brain demonstrated a mass of 2.2×1.2×2.9 cm in size, low to iso signal intensity on T2-weighted images, and high signal intensity on T1-weighted images with no gadolinium enhancement. And cerebrospinal fluid (CSF) space widening around the mass was not found (Fig. 2).
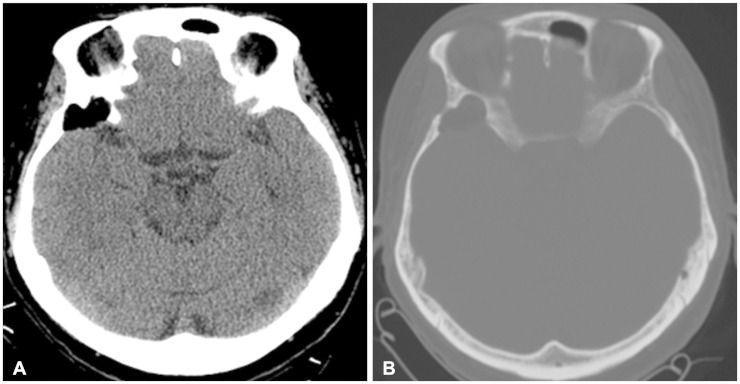 | Fig. 1Computed tomography: soft tissue window (A) and bone window (B) demonstrating a hypodense lesion with bone erosion at right sphenoid ridge, but not communicating with scalp.
|
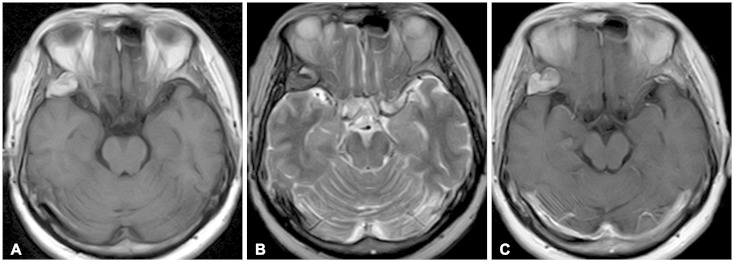 | Fig. 2Magnetic resonance imaging showing an expansile and multilobulated extraaxial mass on right lateral sphenoid ridge with high signal intensity on T1-weighted (A), low to iso signal intensity on T2-weighted (B) and no enhancement on contrast enhancing T1-weighted sequence (C). There was not a cerebrospinal fluid space widening around the mass.
|
Operative findings
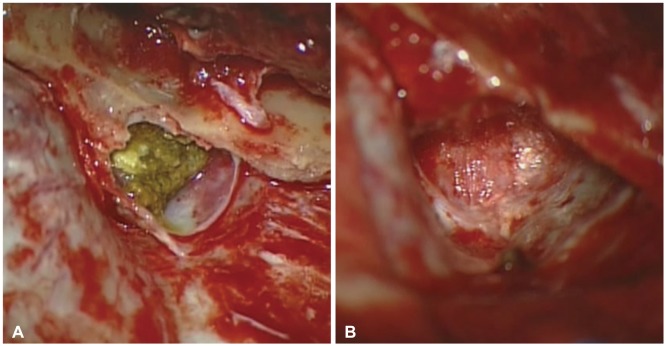
Right pterional craniotomy was performed under general anesthesia. A yellowish and sticky extradural mass containing the capsule was observed at the sphenoidal ridge. The content of the mass was soft and contained desquamated cell debris and hairs. Total resection including the capsule was performed, and the dura was intact after the removal of the mass (Fig. 3).
Postoperative course
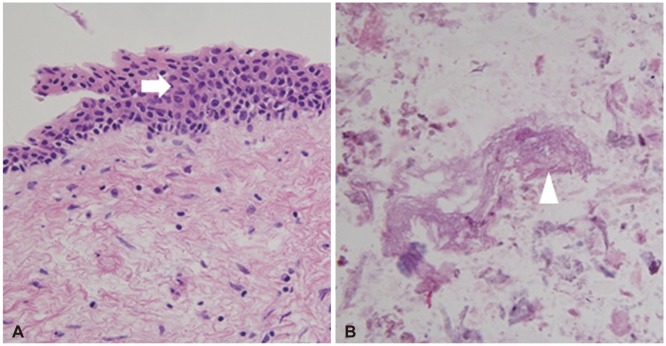
During the postoperative period, the patient had no specific neurologic deficit. Total removal of the mass was confirmed on postoperative MRI. Pathological examination revealed squamous epithelial lining of the cyst and some keratinous contents (Fig. 4), and these findings were consistent with a dermoid tumor. The patient was discharged nine days after operation.
Go to :
DISCUSSION
Dermoid cysts originate from an embryonic ectodermal cell that is involved in the process of primary neurulation during neural tube closure [4,5,6]. Therefore, the contents of dermoid cysts include elements of the dermis such as hair, hair follicles, apocrine, sebaceous, or sweat gland. In the current study, the authors found hairs during tumor resection and keratinous materials in histopathologic findings.
Dermoid cysts primarily occur in intradural regions; however, rare interdural dermoid cysts have also been reported [7]. In addition, although the posterior fossa is the main location for dermoid cysts, a few intradural dermoid cysts originating at the temporal skull base has been reported [1]. Extradural dermoid cysts have been observed in the posterior fossa, diploe of anterior fontanelle, and orbital region in children [1,5,8]. Only one case of a extradural dermoid cyst has been reported in an adult that was located at the paramedian petrous apex accompanied by osseous erosion [9]. And extradural dermoid cysts at the lateral temporal base have been rarely reported so far. Herein, this study has important implications because it is the infrequent case of an intracranial dermoid cyst that is extradural and located at the lateral sphenoid ridge.
Martínez-Lage et al. [5] demonstrated extradural dermoid cysts of the posterior fossa and hypothesized that dermoid cysts of the midline may originate from the cutaneous ectoderm that entered during invagination of dura during development of the falx and tentorium. This hypothesis is difficult to apply to the origin of a lateral extradural dermoid cyst because there is no dural invagination at the lateral temporal region. Two theories for the origin of cells of rare lateral and intradural dermoid cysts are presented here. It has been suggested that dermoid cysts may originate from multipotent embryonic cells or from translocation of epithelial cells that have migrated from the otic vesicles or developing neurovasculature [4]. Although multipotent stem cells were not found in the dura, the possibility of proliferation of these cells cannot be excluded in the formation of extradural dermoid cyst. In addition, during the formation of extradural neurovasculature, epithelial cell migration may also occur. The origin of dermoid cysts is still unknown because multipotent stem cell proliferation or epithelial cell migration occurs in cases of intradural dermoid cysts, and there are only a few reports on these cases [4,6]. In this study, the dermoid cyst could be completely detached from the dura, and no communication with the scalp was found despite its association with the temporal bone erosion on CT scan. The cranium is formed from peripheral mesenchyme during brain development. Although both mesodermal and ectodermal cells are involved in this process, the cartilaginous part of the cranium is formed by the fusion of several cartilages originated from ectodermal cells [10]. Therefore, the possibility that an extradural and lateral dermoid cyst may originate from remnants of ectodermal cells in the skull should be carefully evaluated.
Dermoid cysts are mainly considered hypodense because of fat content with a value of around -100 Hounsfield unit on CT scan [1,9]. In addition, capsular calcification can be observed, and most dermoid cysts do not show contrast enhancement. Dermoid cysts can be detected clearly by high signal intensity on T1-weighted MRI and by low to high signal intensity on T2-weighted images because of the amount of fat present. In some cases of a dermoid cyst, it is difficult to determine whether a lesion is intradural or extradural. Skeletal anomalies such as skull erosion may be a characteristic finding in extradural dermoid cysts [9]. In this study, sphenoid bone erosion was identified on CT scan. In addition, CSF space widening around the mass was not found on MRI. Together with these findings, extradural dermoid cyst should be ruled out for differential diagnosis when bone erosion and CSF space widening are considered.
As a treatment modality, total removal of a dermoid tumor is desirable. However, in the case of intramedullary dermoid cyst [6] which exists in vital structures, attention toward gross total resection is needed because of the risk of a neurological disorder after surgery. Neuromonitoring is sometimes required during surgery. In this case, the tumor could be easily detached from the surrounding structure, and therefore a total removal of the tumor was possible.
Go to :
Conclusion
This study provides the unusual description of an extradural dermoid cyst accompanied by bone erosion located in the lateral sphenoid ridge of the skull. Although various mechanisms can be involved, the origin of lateral and extradural dermoid cyst remains to be determined. In addition, bone erosion and CSF space widening should be considered for the possibility of extradural dermoid cysts when doing differential diagnosis of intracranial mass.
Go to :
 XML Download
XML Download