

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gliomatosis cerebri (GC) is a rare primary brain tumor characterized by diffuse infiltration of the brain by neoplastic glial cells, typically affecting multiple brain areas, but maintaining brain anatomical structure [1]. GC growth patterns uniquely distinguish GC from other primary brain tumors, but the mechanisms involved in GC proliferation remain to be elucidated [1].
Gliomatosis cerebri has been reported worldwide since it was first reported by Nevin [2] in 1938. The World Health Organization (WHO) defines GC as infiltrating tumor cells that affect at least two but generally three cerebral lobes without necrosis [3]. The nature of GC precludes surgical resection, and radical radiotherapy is also considered infeasible in most cases due to its high toxicity [4,5]. Therefore, initially, chemotherapy is used. Either Temozolomide (TMZ) or a combinatorial treatment of Procarbazine, CCNU, and Vincristine (PCV) chemotherapy can be used [6]. Since TMZ exhibits fewer side effects than does PCV chemotherapy, it is traditionally the first choice of drug [6]. We, however, observed good results with PCV chemotherapy in GC. Here, we report our experience regarding PCV chemotherapy in GC and review the literature.
Go to : 
CASE REPORT
Clinical features and radiology findings
A 49-year-old female patient was admitted due to memory disturbances and intermittent headaches, but her Karnofsky Performance Scale (KPS) score was 90 points. She did not have any other past medical history. Her mini-mental status examination (MMSE) score was 25 points. Her global deterioration scale (GDS) score was 4 points. Cranial function tests including assessment of light reflex, ocular motor, and gag reflex were normal. Her neurological examination was also normal, except for minimal cognitive dysfunction.
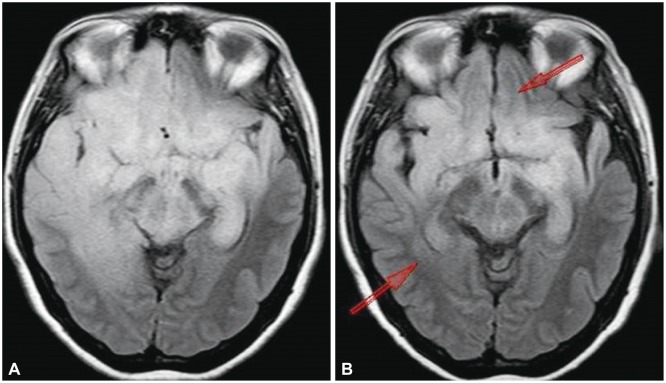
T2-weighted magnetic resonance (MR) image-fluid attenuated inversion recovery showed high signal intensity in both insular lobes, both frontal lobes, both temporal lobes, and the brain stem. A T1-weighted MR image showed iso-signal without enhancement (Fig. 1). It was not enhanced at lesions. It seemed like a tumor with uncertain margins, or inflammatory lesions in both the frontotemporal and insular lobes. Working with only the MR image made the diagnosis difficult.
 | Fig. 1Brain magnetic resonance imaging. A: T1-weighted magnetic resonance image: iso signal in both frontal lobes, both temporal lobes and the brain stem. B: T2 fluid attenuated inversion recovery: high signal in both frontal lobes, both temporal lobes, and brain stem. Brain sulcus is effaced in the tumor lesion. C: T1 enhancement image: no enhancement lesion is in tumor lesion.
|
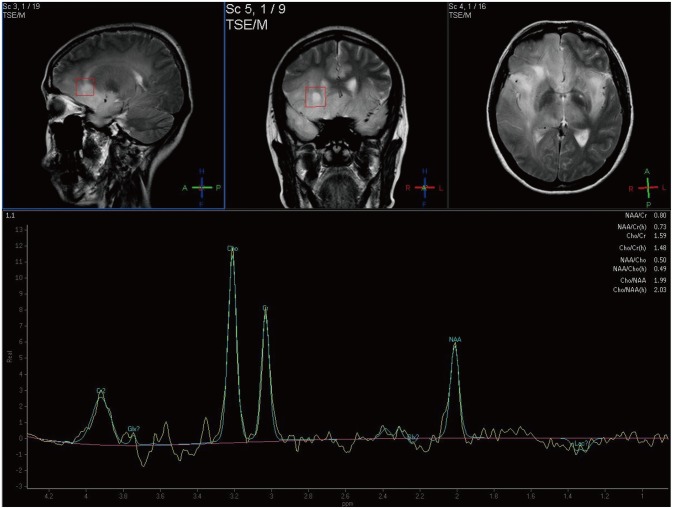
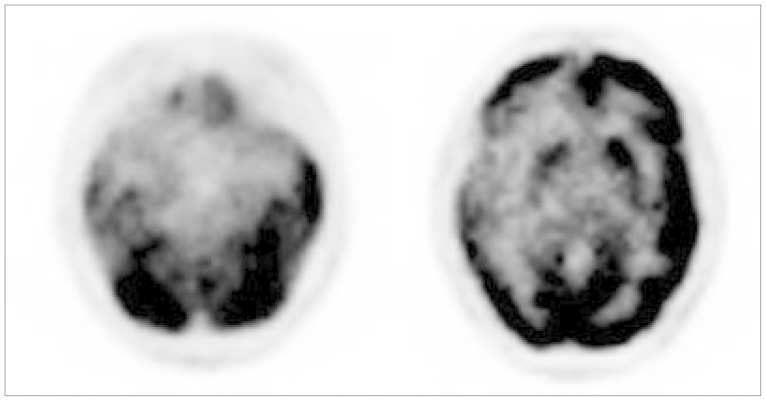
In addition, magnetic resonance spectroscopy (MRS) revealed decreased N-acetyl aspartate, and an increased choline peak (Fig. 2), indicating cell proliferation and a high possibility of malignancy. Positron emission tomography-computed tomography (PET-CT) showed low metabolic activity in the tumor lesion (Fig. 3).
Finally, the lesions in the image were evaluated as a tumor spanning two lobes.
Operation and progress
Widespread surgical resection was considered, but the tumor could not be excised because the lesions were widespread, and their margin was uncertain. Partial surgical resection of non-dominant areas would also have been ineffective, since the lesions were widespread. Additionally, it was not necessary to excise the tumor for intracerebral pressure control or neurologic deficit. First, a stereotactic tumor biopsy was performed from the right frontal part of the tumor lesion, to confirm the diagnosis by pathology.
The glial fibrillary acidic protein immunostaining was well stained; the tumor was therefore of glial cell origin.
In a hematoxylin and eosin staining, cytological atypia was shown, but mitosis, necrosis, and vascular endothelial proliferation were not. In addition, P53 immunostaining was observed, and Ki-67 gene expression was decreased. Overall, this confirmed the astrocytoma WHO grade II diagnosis (Fig. 4).
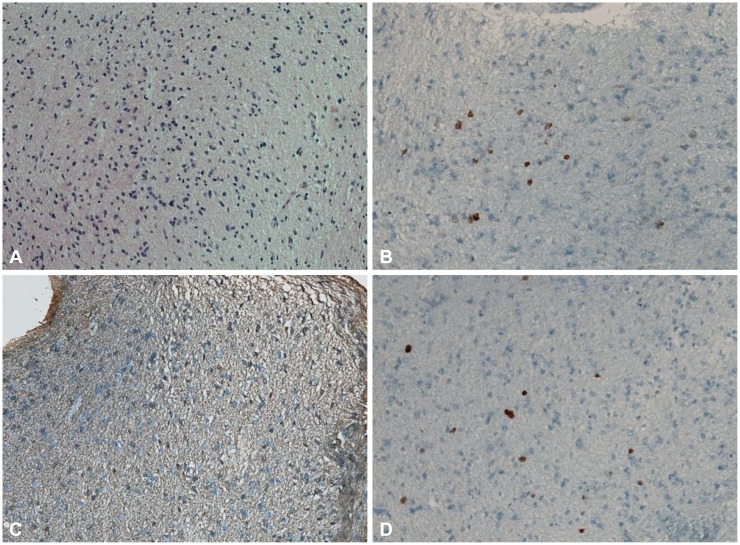 | Fig. 4Pathology. A: Hematoxylin and eosin staining exhibits increased amounts of chromatin and a dismorphic neucleus (×100). B: P53 immunostain: positive (>5%) (×250). C: Glial fibrillary acidic protein immunostain: it is well stained, so the tumor is glial cell origin (×100). D: Ki-67 gene immunostain: decreased gene expression (<5%) (×250).
|
It was judged that radiation therapy and further surgical resection were not appropriate for the patient, considering the cognitive impairment and histology results. TMZ chemotherapy was considered due to its minimal size effects, but it was too expensive for the patient, because it was not covered by insurance. Therefore, we agreed to treat the patient with PCV (CCNU 110 mg/m2, Procarbazine 60 mg/m2, and Vincristine 1.4 mg/m2). The patient had six cycles of PCV chemotherapy (a full dose was applied until the 3rd cycle, and the dose was reduced to 75% for the rest of the cycles) for 16 months. Due to bone marrow suppression, chemotherapy schedule was delayed.
Over the 28 months following the initiation of treatment, the impaired cognitive function improved (GDS 1 points, MMSE 29 points), and the high signal in the right frontal and temporal lobes shown in the T2-weighted MR image decreased (Fig. 5). The patient suffered from side effects from the chemotherapy such as bone marrow suppression [Common Terminology Criteria for Adverse Events (CTCAE) Grade II], dyspepsia (CTCAE Grade II) and peripheral sensory neuropathy (CTCAE Grade I), but they were all successfully managed by medications.
Go to :
DISCUSSION
Gliomatosis cerebri is a unique primary brain tumor. Although GC is classified as a glioma, it is distinctive from glioma in terms of cell proliferation and invasion. It is reported that GC has a less favorable prognosis compared to gliomas of a comparable WHO grade [7]. However, pathophysiology of GC is not yet fully understood, and GC cases with good prognosis factors have only been reported in a small number of literature reports.
Good prognosis factors for GC
Gliomatosis cerebri was a disease with a poor prognosis. Many authors have reported the prognosis and prognosis factors for GC. Taillibert et al. [8] reported that the median survival was 14.5 months, and good prognosis factors were oligodendroglial type, low WHO grade (Grade II) and good performance status (KPS ≥80). Sanson et al. [6] reported that the median survival was 16 months, but only the oligodendroglial type was identified as a having a good prognosis for GC in their study. Chen et al. [9] and Seol et al. [10] reported that the median survival was 18.5 months, and the good prognosis factors were low WHO grade (Grade II) and good performance status (KPS ≥80).
Diagnosis of GC is difficult challenges in diagnosing GC
Diagnosis of GC can be challenging due to the limitations of neuroradiology imaging studies. In GC, structural enlargement and focal or diffuse hypodensity are revealed by a brain CT [11,12]. Minimal or absent enhancement suggest that the blood-brain barrier is intact [11,12]. Once the condition progresses, enhancement can be more prominent. If GC has a minimally infiltrative character, it is sometimes represented as poorly defined lesions and areas of isodensity [13]. This means that a brain CT is non-specific to GC diagnoses. In addition, it is difficult to distinguish GC from leukoencephalopathy, multiple sclerosis and ischemic change [13]. For example, Taillibert et al. [8] reported that several patients with GC were misdiagnosed with other neurological diseases. Brain MR imaging is more sensitive than a brain CT. GC typically shows high signal intensity on T2-weighted images in a diffused pattern without contrast enhancement [11,12]. In addition, the cerebral sulcus can appear flattened, and cerebral ventricles may look compressed [11,12]. Brain MR is also non-specific when assessing GC, making it difficult to differentiate GC from other diseases such as central nervous system inflammatory disease, vasculitis, and leucoencephalopathies [13]. At that time, MRS was helpful. MRS usually reveals raised myo-inositol levels, reduced N-acetyl-aspartate levels and a normal or elevated choline level [14]. In recent years, PET-CT is conveniently utilized in diagnosing GC. Due to a lack of vascular proliferation during tumor cell growth, contrast enhancement is not usually observed in contrast medium MRI, and low metabolic activity is evident in PET-CT [15]. In the reported case, the tumor lesion showed high signal intensity in the T2-weighted image, hypometabolic activity in PET-CT and increased choline/decreased N-acetyl-aspartate in MRS. Based on these findings, the patient was diagnosed with GC.
The diagnosis of GC is usually confirmed by pathological examination of a biopsy. In the reported case, diagnosis of GC was made from the glial fibrillary acidic protein immunostaining result and cytological atypia in the hematoxylin and eosin staining. In addition, a P53 immunostaining and Ki-67 gene expression analysis were helpful for diagnosis of GC. Widely diffused lesions with tumor heterogeneity make it difficult to obtain sufficient sample for biopsy, and accurate histological grading is also challenging in this case.
Treatment of GC
Various treatments have been suggested by retrospective studies. Radiotherapy is a controversial issue. Taillibert et al. [8] reported a high response rate with radiotherapy in GC, but its impact on overall survival was questionable. Elshaikh et al. [16] reported that radiotherapy reduced disease progression, but it was not satisfactory in terms of overall survival. Since GC is a diffused primary tumor, the radiotherapy range covers either the whole brain, or only part of the tumor area. This means that radiotherapy carries the risk of severe toxicity with few benefits in treatment of GC. It has been reported that chemotherapy increases the overall survival rate in GC. Sanson et al. [6] reported TMZ and PCV chemotherapy were effectively resulting in an increase of progression-free-survival and overall survival (16 month, 28.8 month). No significant difference was seen between PCV chemotherapy and TMZ, although TMZ was more tolerable than PCV chemotherapy [6]. Levin et al. [17] also reported the effectiveness of TMZ in GC. They reported that two of three patients in whom PCV therapy was discontinued due to pancytopenia tolerated TMZ well without dose reduction. Therefore, TMZ was recommended as the first-line chemotherapy in GC.
PCV chemotherapy in GC
PCV chemotherapy and TMZ effects in GC were validated by retrospective studies, and another study suggested TMZ was disappointing for the treatment of GC [18]. Prospective studies showed that PCV chemotherapy in low-grade gliomas showed prolonged response without prolonging chemotherapy [19]. A German prospective study evaluating procabazine and CCNU (PC) chemotherapy in GC reported that PC chemotherapy was effective in the treatment of GC and recommended it as the primary therapy [20]. However, in reality, TMZ is much more expensive than PCV chemotherapy. Therefore, it is irrational to treat low grade GC with TMZ in terms of the economic aspect. Hence, PCV chemotherapy can be used as an alternative treatment option for patients with GC. Although this report described only a single patient, the effectiveness of PCV chemotherapy was clinically helpful for GC. The effectiveness of PCV chemotherapy has been validated in a number of studies, despite its more severe side effects when compared to those of TMZ.
In conclusion, with PCV chemotherapy, the impaired cognitive function was improved and the high signal intensity areas in the T2-weighted MR images were reduced. Therefore, PCV chemotherapy can be considered an alternative treatment option for patients with GC who cannot be treated with radiation therapy or other chemotherapies.
Go to :
 XML Download
XML Download