

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Renal cell carcinoma (RCC) accounts for about 1% of systemic cancers and is the most common type of malignancy of the kidney [1,2]. RCC is known for its late recurrence and it is frequently accompanied by systemic diseases that require active medical intervention [2,3]. Patients with brain metastasis from RCC commonly present with headache, confusion, mental change, and seizures, because RCC brain metastases are commonly associated with spontaneous intratumoral hemorrhage and extensive peritumoral edema. Brain metastasis in patients with RCC typically occurs within 3 years from the initial diagnosis [2].
In the present study, we report a case of extremely delayed multiple cerebral metastases of RCC that occurred 18 years after nephrectomy.
Go to : 
CASE REPORT
A 76-year-old woman presented with a protruding scalp mass in the vertex after tripping a couple of days prior to her visit to our emergency department. She had undergone a left nephrectomy at another hospital following the diagnosis of RCC 18 years prior to admission. Magnetic resonance imaging (MRI) showed a large epidural well-enhancing hypervascular tumor in the vertex that compressed the superior sagittal sinus (SSS) downward, with parietal bone destruction. A homogenously well-enhanced tumor was also found along the vein of Galen, with another well-enhanced tumor in the 4th ventricle (Fig. 1A). Brain computed tomography revealed calcification in the mass along the vein of Galen. Abdominal ultrasonography confirmed the left nephrectomy status and no RCC recurrence was evident in either kidneys. Whole body positron emission tomography study showed hypo-metabolism of three brain lesions compared to that of the cerebral cortex, indicating a low grade brain tumor, such as a meningioma. No other abnormal hypermetabolic lesions were found in the rest of the body. Tumor embolization for the vertex mass was performed two days before the surgery. The tumor was supplied by bilateral superficial temporal, occipital, and middle meningeal arteries, and these were successfully embolized using polyvinyl alcohol (Contour, Boston Scientific, USA). The patient underwent a right parietal craniectomy and resection of the vertex mass on Dec. 14, 2005, followed by cranioplasty with bone cement. The tumor was firm and fibrotic and was compressing the SSS. A final histopathological finding was compatible with a metastatic brain tumor from the RCC. The patient underwent fractionated stereotactic radiation therapy for the vertex tumor bed and 4th ventricular mass on Dec. 27, 2005. The tumor found along the vein of Galen was not included in the stereotactic radiosurgery because the MRI findings indicated that it was a meningioma.
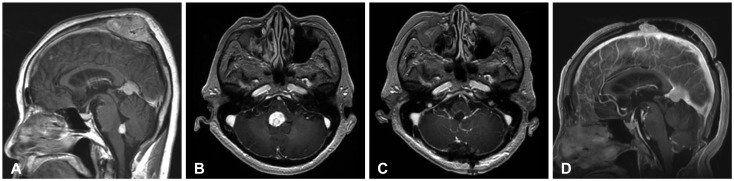 | Fig. 1Series of patient's brain MRI showing the metastatic tumors in different locations. A: Initial sagittal gadolinium-enhanced brain MR image (Dec. 2005) showing a well enhanced large epidural tumor compressing the superior sagittal sinus, with a small tentorial meningioma and another well enhanced 4th ventricle floor mass. B: Axial gadolinium-enhanced brain MR image (Jan. 2008) showing a doubling of the 4th ventricular tumor and increased peritumoral edema. C: Post-operative axial gadolinium-enhanced brain MR image showing gross total resection of the periventricular tumor. D: Follow-up brain MR image (May 2009) showing recurrence of the resected vertex mass.
|
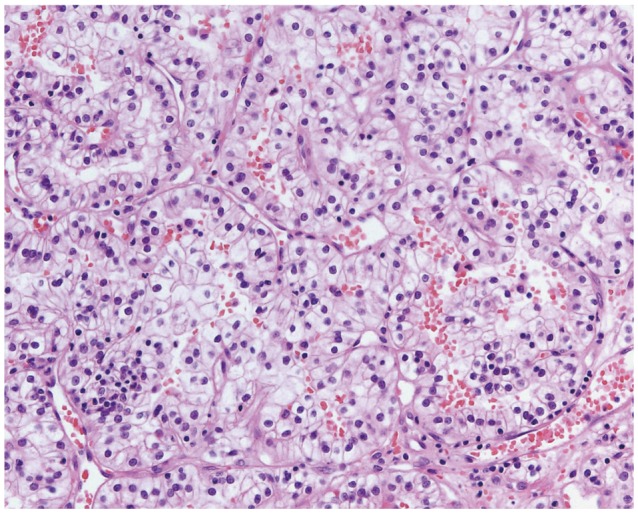
The patient was admitted again on Jan. 31, 2008 for dizziness accompanied by gait disturbance. The brain MRI showed an increase in the size of the 4th ventricular mass with increased peritumoral edema (Fig. 1B). No changes were noted in the sizes of the previously operated vertex mass or the mass along the vein of Galen. No other new intracranial lesions were found. The patient underwent a suboccipital craniotomy and tumor resection for the 4th ventricular mass, which was found to be highly vascular and tightly adhered to the choroid plexus. The lesion was completely removed, and no remaining tumor was observed on the postoperative MRI (Fig. 1C). The histopathological diagnosis was also compatible with metastatic RCC, which was identical with the previous vertex tumor (Fig. 2). The patient recovered without any neurological deficits and received no further adjuvant therapy. A follow-up MRI was taken in our out-patient department after 16 months because she had stopped visiting the hospital after she was discharged. The MRI showed a new small enhancing mass in left cerebellum and recurrence of the vertex mass (Fig. 1D). No changes were seen in the mass along the vein of Galen and 4th ventricular mass. The patient underwent gamma knife radiosurgery for the recurred vertex mass and the cerebellar mass in May, 2009. She survived for about two more years and died in June, 2011.
Go to :
DISCUSSION
RCC accounts for approximately 1% of all adult malignancies, and 25% to 40% of these patients are found to harbor metastasis at the time of initial diagnosis [1,4]. Metastasis to the brain occurs in about 10% of patients with RCC [4,5]. Shuch et al. [6] reported that about 27% of the patients have metastases to the brain at the time of diagnosis of RCC and that the average occurrence of central nervous system (CNS) involvement is 16.9 months from the diagnosis of RCC and non-CNS metastasis.
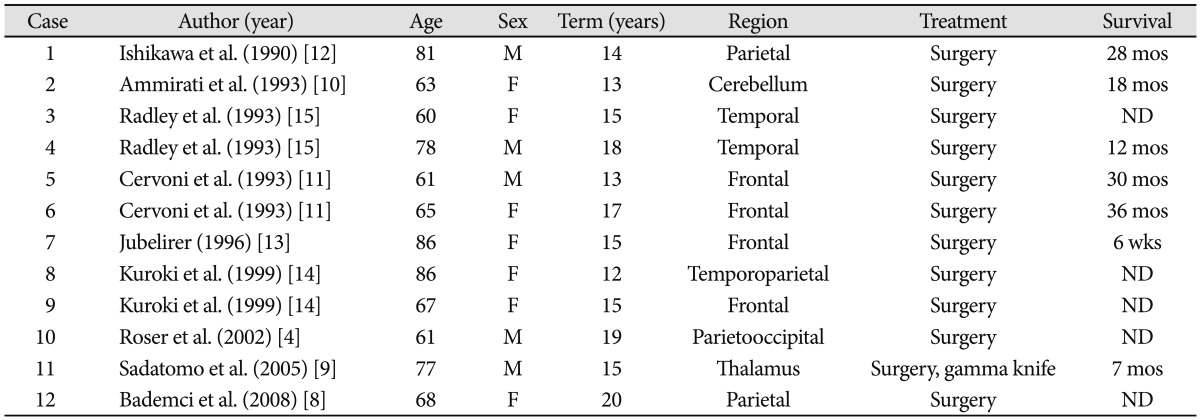
Late recurrence is frequently reported in RCC patients [3,5]. The longest disease free interval, reported by Tapper et al. [7], was 45 years but the reason for this phenomenon is not yet known. Only a few cases of brain metastasis occurring after more than 10 years from the initial diagnosis of RCC have been reported (Table 1) [4,8-15]. Various mechanisms for this type of delayed metastasis have been proposed. One possibility is that growth of a microscopic brain metastasis that occurs in the early stage is so slow that a considerable amount of time elapses before the tumor is diagnosed. This can be correlated with the slow growing nature of RCC, as indicated by its low mitotic index. Another possible explanation is that the growth of a microscopic metastasis starts to accelerate when the host's immune competency is compromised [4,9].
Treatment options for brain metastasis generally include surgical resection, whole brain radiation therapy, and stereotactic radiosurgery [2]. Patients with RCC may experience symptomatic improvement with whole brain radiation therapy, but RCC is considered to be radio-resistant in nature because of its poor response to standard radiation therapy. The 1-year intracranial local control rate is estimated to range from 0% to 14% [16]. In contrast, stereotactic radiosurgery for brain metastasis of RCC reportedly offers good control of tumor growth. Shuto et al. [5] reported that gamma knife radiosurgery on brain metastases smaller than 2 cm brought about 84.3% tumor growth control and 63.8% peri-tumoral edema control for RCC.
Confirmation of the pathology is essential for establishing a further treatment plan for delayed metastasis. Previous reports indicate cases of brain metastasis from RCC that were misdiagnosed as meningiomas because the radiological features of both may be very similar [8]. Resection and pathologic confirmation must be made when the brain lesion is surgically accessible.
Generally, surgical resection plays an important part in the treatment of brain metastasis, especially if the lesion is large, symptomatic, accessible, and surrounded by cerebral edema [2,17]. A long interval between the date of diagnosis of the primary malignancy and the date of CNS metastasis had been considered in previous reports to be an indicator of a favorable prognosis [3,18]. Pathologic confirmation and aggressive treatment must be considered in these delayed brain metastases, since the patients usually have good prognosis after aggressive treatment.
In our case, the patient had been diagnosed with RCC and had undergone nephrectomy at the age of 58. She lived for 18 years without any evidence of recurrence before the brain metastasis was diagnosed. Based on the patient's MRI, differential diagnosis had to be made between the primary intraventricular tumor and brain metastasis. We chose direct surgery for the treatment of the lesion, as well as histopathological confirmation, which revealed the tumor to be a metastatic carcinoma that had originated from the RCC. Adjuvant fractionated stereotactic radiation therapy was performed, as this was available in our hospital.
Go to :
 XML Download
XML Download