

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intradural chondroma is a rare, slow growing, benign intracranial neoplasm, and is very occasionally observed in combination with intratumoral hemorrhage [1]. Most patients present with symptoms of increased intracranial pressure, seizures, or focal neurological deficits. Intradural chondromas usually occur as isolated lesions, but may occur alongside syndromes such as Ollier's disease or Maffuci's syndrome [2]. We report a rare case of intradural chondroma with intratumoral hemorrhage.
CASE REPORT
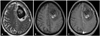
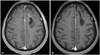
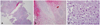
A 55-year-old female visited the emergency room with a complaint of aphasia. She had suffered generalized headaches for 2 months prior to presentation, and had showed memory impairment for 1 month. She had no other relevant medical history and she was right-handed. Neurological examination revealed global aphasia and right side weakness (motor grade I). Her initial brain computed tomography (CT) scan showed an intracranial hemorrhage in the left frontal area. Magnetic resonance imaging showed a 5.9×3.5 cm-sized, non-enhancing mass-like lesion with heterogeneous signal intensity in the left frontal lobe (Fig. 1). Intraoperative findings showed a friable and yellowish tumor adhered to the falx. A frozen biopsy was performed, and the tumor was tentatively diagnosed as a transitional type meningioma. The tumor with intratumoral hemorrhage was totally removed. The bleeding focus of the tumor was uncertain. After surgery, the patient's symptoms were almost totally improved and postoperative CT showed that the tumor had been completely removed (Fig. 2). Histopathological examination confirmed the diagnosis of a chondroma (Fig. 3). The lesion was isolated, not combined with other syndromes as mentioned above. The patient was discharged with only mild dysarthria. Her Karnofsky Performance Scale score was 90 at the time of discharge.
DISCUSSION
Intracranial chondromas are rare benign neoplasm, which comprise only 0.2-0.3% of all intracranial tumors [3]. Intracranial chondromas are thought to arise from ectopic hyaline cartilaginous rests trapped within suture lines [4]. Due to the rarity of intracranial chondromas, few data about this neoplasm are available. Only 3 cases were identified by H. W. Cushing in a previous series of his 2,033 cases [5].
The first patient with intracranial chondroma was reported in 1851, and the first successful surgical resection of an intracranial chondroma was reported in 1982 [6]. Two previous reviews documented 125 and 139 cases of intracranial chondromas, respectively [7,8].
The most common location of intracranial chondroma is the skull base, especially the sellar and parasellar regions [7]. The tumor may also occur in the dura mater of the convexity or the falx, as in our case. However, the exact pathogenesis of intracranial chondroma is uncertain. In the present case, it is most probable that it arose from ectopic hyaline cartilaginous rests trapped within the left coronal suture line or from the falx. Most intracranial chondromas are confined within capsules, as in this case [9].
Recently, Xin et al. [10] reviewed 30 cases of intracranial chondroma that were treated at a single institute, and none showed intratumoral hemorrhaging. Intratumoral hemorrhages often occur in malignant brain tumors such as glioblastomas and metastatic brain tumors, but chondroid tumors rarely develop intratumoral hemorrhages. Only 10 cases of hemorrhages in such tumors have been reported in detail to date, including this case [1].
Chondromas are generally avascular lesions. However, in the present case, the tumor showed intratumoral hemorrhage and a rich blood supply confined within the capsule. Linsen et al. [1] reported a case of an intracranial chondroma with intratumoral and subarachnoidal hemorrhage, and they concluded the rich blood supply was the reason for the hemorrhage. In the present case, the focus of hemorrhage was uncertain, but it was considered to be caused by the rupture of abnormally weak vessels, because intraoperative gross findings of the tumor seemed very friable.
We report a rare case of intradural chondroma with intratumoral hemorrhage. In the present case, imaging findings were not sufficient for diagnosis and the intraoperative finding did not show cartilaginous portions. Histological examination was needed to differentiate chondromas from other tumors, including cases combined with intratumoral hemorrhage. Intradural chondromas may be included in the differential diagnosis of intracranial tumors with acute hemorrhage.
 XML Download
XML Download