

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Non-Hodgkin lymphomas represent only 3% to 4% of all neoplasms in the general population. Primary lymphoma of the bone (PLB) is uncommon, accounting for only 7% of all malignant bone tumors and less than 1% of all non-Hodgkin's lymphomas, and the majority of them involve the pelvis or limb bones [1-3]. Primary cranial vault involvement is rarely reported [4]. We report a case of a cranial vault lymphoma that was found as a frontal scalp mass in an elderly woman.
CASE REPORT
An 81-year-old woman presented with a flatly elevated mid-frontoparietal scalp mass that she noticed one month prior to admission. She was generally healthy and had no remarkable medical history besides taking antihypertensive medication for 20 years. The scalp mass was non-tender, rubbery, hard, non-movable, and its dimensions were 6×4×4 cm.
The patient was completely free from neurological signs and demonstrated no lymphadenopathy, hepatosplenomegaly, or Waldeyer's ring swelling. She had no history of head injury. All of the routine laboratory studies returned with normal results. A plain skull X-ray showed an irregular inner cortical bone margin under the scalp mass, and non-enhanced computed tomography (CT) scans of the brain showed moderately well-defined borders and some osteolytic margins on the inner table of the frontal bone with a permeative extra- and intracranial isodense mass (Fig. 1). T1-weighted image (T1WI) and T2-weighted image (T2WI) magnetic resonance imaging (MRI) of the brain showed an iso- to low signal intensity mass which was well enhanced with gadolininum-Diethylenetriamine pentaacetic acid. MR spectroscopy showed a choline peak in the mass. Digital subtraction angiography showed feeding arteries originating from the bilateral superficial temporal arteries. The tumor also invaded the superior sagittal sinus (Fig. 2).
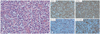
An operation was performed to remove the extra- and intracranial tumor and the involved bone. The tumor was a well-localized, grayish white, soft hypovascular mass that was easily dissected from the surrounding tissue. The dura was diffusely involved but easily separated from the underlying brain without cerebral involvement. Histologic study showed diffusely invading round nuclear immature cells. Immunohistofluorescence staining showed CD20 (+), CD79a (+), and Bcl-2 (+), suggesting a diffuse large B-cell lymphoma. Ki-67 staining was positive in over 90% of nuclei (Fig. 3). Positron emission tomography-CT, chest and abdomen-pelvic CT scans were performed to rule out systemic involvement. The study revealed no systemic involvement except a hypermetabolic lesion in the thyroid, which was diagnosed as a benign follicular nodule.
The patient recovered well and was transferred to the Hemato-Oncology department, where she received three cycles of chemotherapy with CHOP-adriamycin, cyclophosphamide, vincristine, and prednisolone. Nine months after the operation, a follow-up MRI showed no tumor recurrence and the patient remained free from any noticeable symptoms (Fig. 4).
DISCUSSION
PLB is very rare and was first described by Oberling [5] in 1928. Parker and Jackson [6] classified PLB as a unique disease entity in 1939. The diagnostic criteria of PLB are 1) a primary focus in a single bone, 2) a positive histological diagnosis, 3) metastasis to only regional areas on presentation or the primary lesion preceding metastasis [2]. This patient had all of these diagnostic criteria. Causes of PLB have been suggested to be inflammation, trauma, or viral infections, but our patient had none of these [3].
The most common clinical manifestations of calvarial lymphomas are painless scalp masses [2,3,7-9], headaches [2,9], convulsions [1], or focal neurologic signs [1]. But these symptoms and signs are nonspecific, so further radiological and histological studies are needed for a conclusive diagnosis.
The MRI signal intensities are nonspecific and showed variable signal intensities on T1WI and T2WI, but most tumors show unenhanced isointensity and well-enhanced signal intensity [1,10]. Typical radiographic images show a large soft tissue component of the permeative growth or a moth-eaten pattern and less cortical destruction. However, this mimics the appearance of other diseases such as Langerhan cell histiocytosis, osteomyelitis, leukemia, plasmacytoma, Ewing sarcoma, and metastatic cancer [1,7].
During the early stages of calvarial lymphoma, bony change is minimal but gradually extends outward and finally destroys the bone completely [4]. Our patient showed mild bony changes, suggesting that the lesion was in an early stage. The tumor grows rapidly and invades the dura and brain, so early diagnosis is important [4]. Chemotherapy and radiation therapy are the basic treatment modalities for primary calvarial lymphomas, but there are still no standard treatment protocols [4]. Surgery followed by local radiation is the preferred treatment for a single lesion of extranodal disease, but if the lesion is completely removed, radiological follow up without additional treatment may be another option [1]. Generally, surgery with chemotherapy and/or radiation therapy is recommended. In terms of chemotherapy, CHOP is often used [4]. If the patient's lymphoma has widespread dural involvement even after the tumor mass is removed, additional treatment may be provided by the Hemato-Oncology department.
Primary lymphoma of the cranial vault presenting as a scalp mass can easily be missed at the initial diagnosis because of its extreme rarity. However, because of its rapid growth and invasion to the brain, an early diagnosis and active treatment are very important. Although the results of reported cases are variable, the combination of surgery, radiation, and chemotherapy appears to offer favorable outcomes.



 XML Download
XML Download