

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Mortality due to coronary artery disease (CAD) and cerebrovascular accident has increased worldwide over the past few decades. Atherosclerosis is the leading cause of cardiovascular disease (CVD) such as coronary and other atherosclerotic vascular disease. The increase in mortality has been attributed to an increase in the elderly population, a westernized life style, and/or increased chronic disease incidence.12 For the aforementioned reasons, more attention has recently been focused on the aortic disease.3 Although the incidence of aortic aneurysm (AA) has increased with the increase in the elderly population,4 few studies have reported the long-term survival of subjects with AA in Korea. Our objective in this study was to analyze factors affecting the long-term survival of subjects with AA.
METHODS
1. Study population and design
We reviewed the records of patients diagnosed with AA at the Cardiac and Vascular Center, Samsung Medical Center, Seoul, Korea from 1994 through 2004. Subjects consisted of patients with AA (n=267, male=82%) including thoracic aortic aneurysm (TAA, n=52) and abdominal aortic aneurysm (AAA, n=215) confirmed by computed tomography (CT) angiography. TAA and AAA were defined as follows: TAA was AA affecting the thoracic aorta, regardless of abdominal aorta, while AAA was AA affecting only the abdominal aorta. Genetic aorta diseases such as Marfan syndrome and Loeys-Dietz syndrome were excluded. CAD in AA subjects was confirmed by cardiac catheterization, coronary CT, echocardiography, or positron emission tomography. AA repair direct operation or percutaneous endovascular AA repair (AA Revascularized group) (n=161) was performed. Information was obtained by reviewing electronic medical charts. This study was approved by the Samsung Medical Center institutional review board. Informed consent was waived for this retrospective study.
2. Diagnostic criteria
1) Cardiovascular risk factors
Subjects were defined as having hypertension (HT) if they were taking an anti-hypertension drug, had been clinically diagnosed with HT, or had either a systolic blood pressure (SBP) ≥140 mmHg or a diastolic blood pressure (DBP) ≥90 mmHg.5 Subjects who met one of the following requirements were defined as having diabetes mellitus (DM): taking an oral hyperglycemic agent, using insulin, clinical diagnosis of diabetes, or a fasting plasma glucose >125 mg/dL.5 Subjects were defined as dyslipidemia if they met one of the following requirements: diagnosis of hypercholesterolemia, medication history for hypercholesterolemia or total cholesterol (TC) >200 mg/dL or low density lipoprotein (LDL) >130 mg/dL.5 The criterion for obesity based on body mass index (BMI) was BMI ≥ 25.6 A patient who had smoked within a year prior to the study was defined as a smoker. The estimated glomerular filtration rate (eGFR), which is used as an indicator of kidney function, was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. The CKD-EPI equation is eGFR = 141 × min (serum Cr /κ, 1)α × max (serum Cr /κ, 1)-1.209 × 0.993Age × 1.018 [if female], where κ is 0.7 for females and 0.9 for males, α is -0.329 for females and -0.411 for males, min indicates the minimum of serum Cr /κ or 1, and max indicates the maximum of serum Cr /κ or 1. Multiplication factors for race and sex are incorporated into the intercept, which results in different intercepts for different age and sex combinations. The National Kidney Foundation Kidney Disease Outcome Quality Initiative defines chronic kidney disease (CKD) as an eGFR <60 mL/min/1.73m2.
3. Statistical analysis
General and clinical characteristics of AA subjects are reported as means±standard deviations (SD) for continuous variables and percentages for categorical variables. Kaplan-Meier analysis was used to plot survival curves for AA subjects. Kaplan-Meier method was also used to compare survival among patients with AA at different sites or in the presence of CAD using log-rank tests. Multiple cox proportional hazards analysis was carried out using the variables of age, gender, SBP, DBP, fasting plasma glucose, triglyceride, high density lipoprotein, eGFR, smoking, BMI, AA revascularized group, and AA maximum size.
RESULTS
The mean age of AA subjects was 68.7 (±8.1) years. The proportion of patients older than 65 years was 70.8%. The proportion of males was 82%. The proportion of cardiovascular risk factors in the patient population was as follows: over 60% had HT, over 40% had dyslipidemia or were smokers, over 30% had CKD, and over 20% had DM or were obese. The proportion of CAD comorbidity was 19.9% (Table 1).
Five- and 10-year survival rates for all subjects were 89.8% and 82.6%, respectively. The 5- and 10-year survival rates were 90.2% and 83.3% for AAA patients and 86.4% and 76.8% for TAA patients, respectively (p=0.250). The 5- and 10-year survival rates were 88.7% and 81.9% in non-CAD subjects versus 92.6% and 86.6% in CAD subjects, respectively (p=0.490). And for AA revascularized group versus non-revascularized group, the 5- and 10-year survival rates were 92.3% and 84.9 % in AA revascularized group versus 86.4% and 79.5% in non-revascularized group, respectively (p=0.173) (Fig. 1).
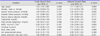
Adjusted hazard ratios (HRs) of age was 1.11 {95% confidence interval [CI] 1.04-1.21} and adjusted HRs of smoking was 3.07 (95% CI 1.26-7.90) in smoking for AA subjects (Table 2). However, adjusted HRs of gender, SBP, DBP, fasting plasma glucose, triglyceride, high density lipoprotein, eGFR, BMI, AA revascularized group, and AA maximum size was not significant association.
DISCUSSION
The old age group and the current smoking group showed higher risk for death in AA patients. These findings are consistent with those of previous studies that smoking is a predictor for AA patients.78910 AA development was contributed endotherial cells.11 Endotherial cells respond to a number of stimulating factors such as smoking.12 Therefore, aggressive non-smoking education program should be applied in smoking AA patients. However, a study in an England cohort from 1997 through 2010 showed that smoking was not associated with cardiac death.13 Mechanism of underlying the association between older age and development of AA might be related to aortic wall changes. With aging, the vascular wall will gradually lose its elasticity, resulting in aortic dilatation from which mechanical forces will be conveyed to collagen within the aortic wall. Subsequent changes in collagen due to remodeling will lead to a stiffer and less compliant vessel.14 These findings differ from those for HT,89 DM,15 and BMI-defined obesity.9 Dyslipidemia16 and CKD may be involved in the pathophysiologic mechanism of development due to AA. In previous studies, calcium-channel blockers were an independent risk factor for the presence of an AAA and were associated with increased arterial aortic wall stiffness.17 Angiotensin-converting-enzyme inhibitors were associated with decreased stiffness and greater collagen turnover.17 And, beta-blockers may be used to slow the growth rate of an AA.18
The 5- and 10-year survival rates for Korean AA patients were over 80%. AA with CAD, AA without CAD, and AAA subjects also showed over 80% survival rate over 5 and 10 years. Patients with TAA had the lowest 10-year survival rate of 76.8%. Furthermore, the 5- and 10-year survival rates were 92.3% and 84.9% in AA revascularized group and 86.4% and 79.5% in non-revascularized group, respectively. In Korea, 21,301 echocardiography devices were available at 62,853 medical institutions registered with the National Health Insurance Service in 2013.19 This easy accessibility to clinics or hospitals and earlier health examination may have contributed to the higher AA survival rates in Korea. Also, it is important to educate patients and to follow AHA/ACC guidelines for secondary prevention, especially in those patients with coronary and other atherosclerotic vascular diseases in 2006.20
Our study showed the proportion of male patients was higher than that of female patients. This result is consistent with United States AAA study.21 Their study showed that the ratio of male vs female was 4:1. In addition, they revealed that female are protected from AAA formation not only in human22 but also in animal model.2324
This study had several limitations. First, the study was conducted retrospectively at a single center, which may have caused selection bias. We were also unable to eliminate the possibility of information bias when collecting medical records from the medical charts of the subjects and laboratory results. Second, we did not consider other CAD risk factors such as CRP,25 homocysteine,26 lipoprotein(a),27 fibrinogen,28 physical activity, nutrition, socioeconomic position, or health behavior variables in this study. Furthermore, we were unable to analyze smoking details because we grouped the patients only into current smoking and ex-smoker or none. Therefore, risk factors of atherosclerosis for prediction of CVD should be confirmed in further prospective cohort studies. We also suggest active non-smoking education program should be applied in smoking AA patients. Third, we could not separately analyze cox proportional hazard model for AAA and TAA due to their small sample size.
CONCLUSIONS
We found that age and smoking were associated with increased risk of death in AA patients in Korea. The proportion of male and older age was over two thirds, and the 10-year survival rate for AA patients in Korea was over 80%. Especially, the 10-year survival rates of AA revascularized group were over 85%.


 XML Download
XML Download