

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Heart failure (HF) is a common chronic disease that increases morbidity, mortality, and healthcare expenditure.12 Patients with HF are at high risk for recurrent symptomatic exacerbations leading to hospitalization or death.3 Many factors are related with HF, including hypertension (HTN), diabetes mellitus (DM), coronary artery disease (CAD), and valvular heart disease. Since the incidence of myocardial infarction (MI) increases, ischemic heart failure (IHF) may be considered as an important factor that can influence long term prognosis of MI. The incidence of HF after MI varies in the range from 3% to 53%,45 but clinical importance of its incidence in prognosis is well-known. The stage of HF is classified by left ventricular systolic function based on left ventricular ejection fraction (LVEF).6 Underlying process of neurohormonal abnormalities and noncardiac comorbidities may be related with disease progression of heart failure. Some neurohormonal antagonists such as angiotensin-converting enzyme inhibitor (ACEI), angiotensin receptor blocker (ARB), beta-blocker, aldosterone antagonist, and cardiac resynchronization therapy (CRT) have been widely used to improve clinical outcomes in patients with HF and reduced LVEF.7 Several factors like C-reactive protein (CRP), B-type natriuretic peptide (BNP), cardiac troponin-T are possible predictors of heart failure.89 The purpose of this study is to define the effect of LVEF change ratio on long-term major adverse cardiac events (MACEs) in patients with acute myocardial infarction (AMI).
METHODS
1. Patient population
A total of 1,188 patients from November 2005 to December 2006 who had completed 5-year follow-up and had undergone 2-dimensional (2D) echocardiography follow-up after one year at Chonnam National University Hospital (CNUH) were included in this study population.
2. Medical treatment and percutaneous coronary intervention (PCI) procedure
All patients initially received 100 mg or higher dose of aspirin and 300 to 600 mg loading dose of clopidogrel, and heparin. The maintenance dose was aspirin 100 mg/day and clopidogrel 75 mg/day. Aspirin and clopidogrel were administered to all patients for longer than 6 months according to existing guidelines. The postintervention medications included aspirin, clopidogrel, beta-blockers, ACEI, and ARB unless contraindicated. Coronary artery stenting was performed using the standard technique. The decision for predilatation, direct stenting, postadjunctive balloon inflation, and the administration of glycoprotein IIb/IIIa receptor blockers was left to the discretion of individual operators. Clinical follow-up was performed at 1, 6, 12, 60 months and when anginalike symptoms occurred. Follow-up 2D echocardiography was performed at 12 to 24 months after AMI. Left ventricular mass index (LVMI) was calculated with Devereux's formula.10 LVEF change ratio was calculated as below:
3. Study Definition and End Points
The diagnosis of AMI was made by the presence of characteristic clinical presentation, serial changes on electrocardiogram suggesting infarction, and elevated cardiac enzymes. Primary end point was the composite of MACEs during the 5 years of clinical follow-up. MACEs was defined as the composite of all-cause death, MI, and repeated PCI or coronary artery bypass grafting (CABG). All-cause death was considered as a cardiac death unless a non-cardiac death was clearly defined. Recurrent MI was defined as recurrent symptoms with new electrocardiographic changes compatible with MI or elevated cardiac enzymes at least twice the upper limit of normal. Target-vessel revascularization (TVR) was defined as any repeated intervention driven by the lesions located in the treated vessel within and beyond the target limits. Secondary end points were individual components of the primary end point including cardiac death, all-cause death, recurrent MI, and coronary revascularization procedures. Ischemic heart failure was defined with LVEF less than 45% according to previous studies.11 Progression to LVD (PLVD) was defined as LVEF change ratio less than 0%. Cardiac biomarker cut-off values used to analyze risk factors in PLVD were divided according to ROC curve.
4. Statistical analysis
All statistical analyses were done with SPSS 19.0 (Statistical Package for the Social Sciences, SPSS-PC Inc, Chicago, Illinois). For continuous variables, the differences between groups were evaluated by an unpaired t-test or Mann-Whitney rank-sum test. For discrete variables, differences were expressed as counts and percentages and were analyzed with a chi-square test (or Fisher's extract) among groups. Cox proportional hazards regression was used to compute hazard ratios (HRs) and odd ratios (ORs) for estimation of each end point. HRs were adjusted for propensity score and important risk covariables that had significant effects (p<0.01) in the univariate analysis for clinical outcomes. The risk factors for PLVD were analyzed by using linear logistic regression. All analyses were 2-tailed test with a clinical significance level of 0.05.
RESULTS
1. Baseline characteristics and laboratory findings
A total of 1,188 patients with AMI were analyzed in this study, and divided into two groups according to initial LVEF [group I (LVEF<45%); n=280, group II (LVEF≥45% group); n=908]. The baseline characteristics are presented in Table 1. The mean age was older (66.0±12.4 vs. 62.1±12.3, p=0.01), and DM was more common in group I (107(35.7%) vs. 234(25.2%), p=0.01). However, body mass index (BMI) (19.6±9.1 vs. 23.4±5.3, p=0.01) was lower in group I. ST-elevation MI (STEMI) was more common in group I (216(71.1%) vs. 593(63.6%)), and Non-ST elevation MI (NSTEMI) was more common in group II (88(28.9%) vs. 339(36.4%)) (p=0.018). Cardiac arrests were more frequent in group I (28(9.2%) vs. 19(2.0%), p=0.01). Initial laboratory findings also showed several differences in both groups. Glucose, creatinine, creatine kinase (CK), CK-MB, troponin-I, troponin-T, high sensitivity C-reactive protein (hsCRP), pro-B-type natriuretic peptide (proBNP) were higher in group I (p=0.01). Analysis of angiographic findings showed no difference between group I and II in prevalence of multi-vessel disease, American College of Cardiology/American Heart Association (ACC/AHA) lesion type, location of culprit lesions, and stent type (Table 2).
2. Clinical characteristics in patients with ischemic heart failure
All of 1,188 patients had undergone follow-up 2D echocardiography after one year, and were divided into 3 groups: group A (increased LVEF change ratio, n=626, 52.6%), group B (decreased LVEF change ratio less than 20%, n=414, 34.8%), and group C (decreased LVEF change ratio more than 20%, n=148, 12.4%). Baseline characteristics showed difference among groups in age (63.2±12.7 years vs. 65.4±11.1 years vs. 67.9±12.6 years, p=0.027), follow-up LVEF (60.4±12.3% vs. 47.9±12.1% vs. 39.9±11.6%, p=0.001), follow-up LVMI (244.1±63.9 g/m2 vs. 271.9±64.7 g/m2 vs. 291.7±63.2 g/m2, p=0.010), atrial arrhythmia (including atrial fibrillation and atrial flutter) [21(4.4) vs. 18(5.8) vs. 18(12.1), p=0.041], follow-up GFR (75.0±30.1 ml/min•1.73 m2 vs. 68.2±38.3 ml/min•1.73m2 vs. 57.1±27.2 ml/min•1.73m2, p=0.038). No significant difference was observed in coronary angiographic findings (Table 3).
3. Clinical outcomes
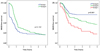
Patients were divided into two groups according to initial LVEF, and long-term MACEs occurred in 46 (16.4%) patients of group I and 143 (15.7%) patients of group II (p=0.152, Fig. 1). 5-year MACEs according to LVEF change ratio showed interesting outcomes. 5-year MACEs occurred in 62 (9.9%) patients of group A, 83 (20.0%) patients of group B, and 44 (29.7%) patients of group C. Early MACEs (within one month) rates were similar between group A and B, but was apparently lower in group C. However, the long-term prognosis of each group showed significant difference (p=0.041, Fig. 1).
Multivariate analysis for long-term MACEs showed that initial low EF (<45%) was not a risk factor, (HR, 1.686; 95% index (CI), 0.861-2.862, p=0.065), but the LVEF change ratio was a strong risk factor for long-term MACEs (HR, 3.731; 95% CI, 2.039- 6.828, p=0.001).
We also compared long-term MACEs in initial low LVEF patient group and low LVEF patient group at follow-up period. We divided patients into 4 groups (<15%, 15-25%, 25-35%, 35-45%) by their initial LVEF and follow-up LVEF. The long-term MACEs in each group showed no significant difference (p>0.05, Fig. 2).
4. Multivariable analysis for progress to left ventricular dysfunction (PLVD)
Multivariable analysis showed that PLVD in this study population was associated with significantly poor clinical outcomes in the elderly [>75 years old; OR, 1.701; 95% CI, 1.325-1.813], female sex (OR, 2.557; 95% CI, 1.186-5.512), DM (OR, 1.289; 95% CI, 1.176-2.143), atrial arrhythmia (OR, 2.191; 95% CI, 1.508-9.455), increased LVMI>20% in follow-up 2D echocardiography (OR, 1.862; 95% CI, 1.503-1.977), decreased GFR (<50 ml/min)(OR, 1.631; 95% CI, 1.578-3.417), multi-vessel disease (OR, 1.937; 95% CI, 1.588-2.492), increased pro-BNP (>5,000 pg/mL) (OR, 1.814; 95% CI, 1.672-7.132), and increased hs-CRP (>3.0 mg/dL) (OR, 2.144; 95% CI, 1.919-8.133). Administration of ACEI or ARB (OR, 0.485; 95% CI, 0.468-0.854) was associated with preventing PLVD. Interestingly, initial LV failure (EF<45%) had no significant relationship with decrease in LVEF.
DISCUSSION
IHF is commonly known as the most important prognostic factor in AMI, and many trials and meta-analysis were performed to find predictive factors of IHF in AMI patients.1213 We followed 1,188 patients with AMI for 5 years, and total MACEs occurred in 189 (15.9%) patients during follow-up period. Initial low LVEF was not a risk factor for long-term MACEs, but decreased LVEF change ratio more than 20% was a strong risk factor. We found that multiple predictive factors were associated with PLVD including age over 75 years, female, atrial arrhythmia, increased LVMI more than 20% in follow-up echocardiography, acute renal failure (GFR decrease by 50%), multi-vessel disease and increased pro-BNP (>5,000 pg/mL), and increased hs-CRP (>3.0 mg/dL). All of these results have been discussed as predictive factors for IHF in many previous studies,1415161718 and we confirmed that these factors were associated with long-term MACEs in our study population. However, initial low LVEF was not related to follow-up LVEF reduction. Decreased follow-up LVEF affected long-term MACEs while initial low LVEF did not. Incidence of early MACEs between group A and B were comparable, but long-term MACEs were significantly different among group A, B, and C.
LVEF has been widely studied for the prognosis of HF and risk of sudden cardiac death,192021 but we cannot predict prognosis of HF with LVEF alone. The role of initial low LVEF as a predictor of long-term MACEs is not well-established. Although initial low LVEF is not associated with follow-up LVEF reduction in our study, we hypothesized that intensive medical treatment to all AMI patients including patients with initially preserved LVEF might improve long-term clinical outcomes. The controllable predictive factors of heart failure were atrial arrhythmia, LVMI, and acute renal failure. Intensive medical treatment for patients with permanent atrial arrhythmia, initially decreased GFR, and increased LVMI more than 20% in follow-up 2D echocardiography after one year can reduce incidence of long-term MACEs.
Atrial arrhythmia is commonly known as a risk factor and poor prognosis factor for MI.2223 Beukema RJ, et al. reported that new onset of atrial fibrillation after PCI for MI as an independent poor prognostic factor.24 Possibly, new onset atrial fibrillation after PCI is a symptom of failed reperfusion and a sign of heart failure. Therefore, we would recommend to closely observe atrial arrhythmia after PCI. If atrial arrhythmia happens after PCI, atrial arrhythmia needs to be controlled in order to reduce incidence of long-term MACEs.
The effects of renal function in MI have been widely studied, and its clinical significance is well-known as a risk factor and a prognostic factor.252627 Acute renal failure and contrast-induced nephropathy (CIN) in PCI can cause chronic renal failure or end-stage renal disease (ESRD) which may highly increase short-term and long-term mortalities.
Left ventricular hypertrophy (LVH) is one of the strongest risk factors of death and major cardiovascular events. It is a good predictive marker of the long-term exposure of the myocardium to environmental risk factors like hypertension and volume/salt overload, metabolic problems including insulin resistance, and genetic factors.28 LVH is associated with higher cardiovascular risk and is commonly associated with obesity, hypertension, ESRD and demonstrates an adaptation of the heart to comply with increased burden of pumping.2930 Elderly patients with increased LV mass were shown to be related to higher incidence of MI even though some patients were asymptomatic.31 Anti-hypertensive treatment including ACEI/ARBs, and spironolactone were reported to decrease LV mass and reduced LVH effectively.323334 Statin seems to be effective in regressing LVH, but its efficacy in decreasing LV mass requires further studies.3536
Low LVEF after AMI is a risk factor of MACEs including cardiac arrhythmia and sudden cardiac death.3738 It is also found in our study that group C showed significantly higher prevalence of atrial arrhythmia than other groups, while group I and II had no significant difference. Thus, decreased follow-up LVEF after AMI appears to be more significant risk factor for long-term MACEs than initial low LVEF. Therefore, intensive medical treatments to prevent reduction in LVEF are required for every AMI patients even though they had initially preserved LVEF.
The present study has several limitations. First, the database of this study was obtained from a single center. Therefore, we could not ignore regional and procedural limitations among patients. Second, the number of study population is 1,188 patients, which may not be a sufficient number of patients to represent disease subjects. Third, this study was analyzed retrospectively. The non-randomized nature of our registry data could have resulted in potential selection bias, although most of confounders were included in the multivariate regression analysis model. A large scale prospective randomized study is needed to clarify predictors of IHF and causes of long-term MACEs. Fourth, We described that multivariate analysis for long-term MACEs showed that initial low EF (<45%) was not a risk factor (HR, 1.686; 95% CI, 0.861-2.862, p=0.065). However, as shown by the p value, the results may be marginally significant. Some patients might have died before the follow-up 2D echocardiography or might have lost to follow-up due to limitation of retrospective study design. If data of these patients were included, initial low EF may have turned out to be a risk factor of MACEs. Therefore, further prospective study is needed to determine the relationship between LVEF and MACE. Fifth, initial and 1 year follow-up medications showed no significant difference, but medication change after 1 year clinical follow-up was not considered. This could influence long-term MACEs; therefore, further studies about the relationship between long-term medications and LVEF changes over 1 year are recommended. Sixth, five patients who experienced AMI from November 2005 to December 2006 were treated thrombolysis. But two patients did not have 2D echocardiography follow-up, and three patients had clinical follow-up in other hospital after discharge. In these patients, we could not compare the efficacy between thrombolysis and PCI.
CONCLUSIONS
The present study suggests the importance of LVEF changes in long-term MACEs. Initial low LVEF is not a risk factor for long-term MACEs, but changes in LVEF have more influence in long-term MACEs. The risk factors of PLVD in AMI are old age, female sex, increased LVMI, acute renal failure, atrial arrhythmia, absence of ACEI/ARB, multivessel disease, increased pro-BNP, and increased hs-CRP. Patients with these factors tend to lead to severe LV failure and demonstrate low MACE-free survival rates. Since initial LVEF may not be a predictive factor for LVD, we recommend intensive medical treatment to patients with preserved LVEF patients and initially decreased LVEF patients.




 XML Download
XML Download