

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Objective
To investigate the usefulness of cardiac biomarkers in the evaluation of prognosis and cardiac involvement (CI) in patients with acute aortic syndrome (AAS).
Methods
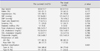
A total of 260 AAS patients with the measurements of cardiac biomarkers were divided into 2 groups; the survived (n=215, 60.6±13.7 years, 110 males) vs the dead (n=45, 64.5±13.6 years, 19 males). N-terminal pro-B-type natriuretic peptide (NT-proBNP), cardiac specific troponin-I (cTnI), C-reactive protein (CRP), creatinine kinase (CK), MB fraction of CK (CK-MB), and D-dimer were compared.
Results
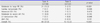
NT-proBNP and D-dimer were significantly elevated in the dead group than in the survived group (3558.7±5497.2 vs 949.9±2307.3 pg/mL, p<0.001, 4.5±5.1 vs 2.0±3.2 ug/mL, p<0.001, respectively). CI was observed in 59 patients (22.7%), and NT-proBNP was significantly elevated in patients with CI than in patients without CI (2497.7±4671.3 vs 722.5±1489.1 pg/mL, p=0.034). In univariate analysis, Stanford type A, CI, NT-proBNP, and D-dimer were significantly associated with mortality, but NT-proBNP was the only significant independent predictor of mortality in multivariate analysis. By receiver operating characteristic curve analysis, the optimal cut-off value to predict mortality was 517.0 pg/mL for NT-proBNP (area under the curve 0.797, sensitivity 86.7%, specificity 71.7%).
Figures and Tables
 | Fig. 1Receiver operating characteristic curve analysis to predict mortality in acute aortic syndrome. Asterisk indicates the optimal cut-off value. NT-proBNP; N-terminal pro B-type natriuretic peptide.
|
Table 1
Baseline clinical characteristics between the groups
![]()
Table 2
Echocardiographic findings between the groups
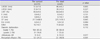
Values are means±SD.
LVEDD; left ventricular end-diastolic dimension, LVESD; left ventricular end-systolic dimension, LVEF; left ventricular ejection fraction, E; early diastolic mitral inflow velocity, A; late diastolic mitral inflow velocity, DT; deceleration time, Em; early diastolic velocity of septal annulus, AR; aortic regurgitation
![]()
Table 3
Cardiac biomarkers and mortality between the groups

![]()
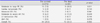
Table 4
Differences of cardiac biomarkers according to the Stanford classification of acute aortic syndrome

![]()
Table 5
Differences of cardiac biomarkers according to the cardiac involvement in patients with acute aortic syndrome

![]()
Table 6
Cardiac involvement and Stanford classification
![]()
Table 7
Cardiac involvement between the survived and the dead
![]()
Table 8
Independent predictor of mortality in acute aortic syndrome
![]()
References
1. Golledge J, Eagle KA. Acute aortic dissection. Lancet. 2008; 372:55–66.

2. Song JK, Kang SJ, Song JM, Kang DH, Song H, Chung CH, et al. Factors associated with in-hospital mortality in patients with acute aortic syndrome involving the ascending aorta. Int J Cardiol. 2007; 115:14–18.
3. Vasan RS. Biomarkers of cardiovascular disease: molecular basis and practical considerations. Circulation. 2006; 113:2335–2362.
4. McLean AS, Huang SJ. Cardiac biomarkers in the intensive care unit. Ann Intensive Care. 2012; 2:8–18.
5. Mir MA. Aortic dissection--in pursuit of a serum marker. Am J Emerg Med. 2008; 26:942–945.
6. Wen D, Zhou XL, Li JJ, Hui RT. Biomarkers in aortic dissection. Clin Chim Acta. 2011; 412:688–695.
7. Sugano Y, Anzai T, Yoshikawa T, Satoh T, Iwanaga S, Hayashi T, et al. Serum C-reactive protein elevation predicts poor clinical outcome in patients with distal type acute aortic dissection: association with the occurrence of oxygenation impairment. Int J Cardiol. 2005; 102:39–45.
8. Linder N, Treitl M, Nikolaou K, Juchem G, Pichlmaier M, Reiser MF, et al. Acute aortic syndrome. Radiologe. 2012; 52:844–848.
9. Parthenakis F, Koutalas E, Patrianakos A, Koukouvas M, Nyktari E, Vardas P. Diagnosing acute aortic syndromes: the role of specific biochemical markers. Int J Cardiol. 2010; 145:3–8.
10. Tokita Y, Kusama Y, Kodani E, Tadera T, Nakagomi A, Atarashi H, et al. Utility of rapid D-dimer measurement for screening of acute cardiovascular disease in the emergency setting. J Cardiol. 2009; 53:334–340.
11. Evangelista Masip A. Progress in the acute aortic syndrome. Rev Esp Cardiol. 2007; 60:428–439.
12. D'Aloia A, Faggiano P, Brentana L, DeiCas L. D-dimer serum levels in a case of type B aortic dissection A rapid test for the early diagnosis of acute aortic disease? J Cardiovasc Med (Hagerstown). 2006; 7:216–218.
13. Wen D, Wu HY, Jiang XJ, Zhang HM, Zhou XL, Li JJ, et al. Role of plasma C-reactive protein and white blood cell count in predicting in-hospital clinical events of acute type A aortic dissection. Chin Med J (Engl). 2011; 124:2678–2682.
14. Sbarouni E, Georgiadou P, Marathias A, Geroulanos S, Kremastinos DT. D-dimer and BNP levels in acute aortic dissection. Int J Cardiol. 2007; 122:170–172.
15. Sodeck G, Domanovits H, Schillinger M, Janata K, Thalmann M, Ehrlich MP, et al. Pre-operative N-terminal pro-brain natriuretic peptide predicts outcome in type A aortic dissection. J Am Coll Cardiol. 2008; 51:1092–1097.
16. Cho JR, Shin S, Kim JS, Ko YG, Hong MK, Jang Y, et al. Clinical characteristics of acute aortic syndrome in Korean patients: from the Korean multi-center registry of acute aortic syndrome. Korean Circ J. 2012; 42:528–537.
17. Tsai TT, Nienaber CA, Eagle KA. Acute aortic syndromes. Circulation. 2005; 112:3802–3813.
18. Yamashita T, Seino Y, Ogawa A, Ogata K, Fukushima M, Tanaka K, et al. N-terminal pro-BNP is a novel biomarker for integrated cardio-renal burden and early risk stratification in patients admitted for cardiac emergency. J Cardiol. 2010; 55:377–383.
19. Emdin M, Vittorini S, Passino C, Clerico A. Old and new biomarkers of heart failure. Eur J Heart Fail. 2009; 11:331–335.
20. Tschöpe C, Kasner M, Westermann D, Gaub R, Poller WC, Schultheiss HP. The role of NT-proBNP in the diagnostics of isolated diastolic dysfunction: correlation with echocardiographic and invasive measurements. Eur Heart J. 2005; 26:2277–2284.
21. Kehl DW, Iqbal N, Fard A, Kipper BA, De La Parra Landa A, Maisel AS. Biomarkers in acute myocardial injury. Transl Res. 2012; 159:252–264.
22. Bonnefoy E, Godon P, Kirkorian G, Chabaud S, Touboul P. Significance of serum troponin I elevation in patients with acute aortic dissection of the ascending aorta. Acta Cardiol. 2005; 60:165–170.
23. Nienaber CA, Powell JT. Management of acute aortic syndromes. Eur Heart J. 2012; 33:26–35b.
24. Imoto K, Uchida K, Karube N, Yasutsune T, Cho T, Kimura K, et al. Risk analysis and improvement of strategies in patients who have acute type A aortic dissection with coronary artery dissection. Eur J Cardiothorac Surg. 2013; 44:419–424.
25. Ohlmann P, Faure A, Morel O, Petit H, Kabbaj H, Meyer N, et al. Diagnostic and prognostic value of circulating D-dimers in patients with acute aortic dissection. Crit Care Med. 2006; 34:1358–1364.
26. Ranasinghe AM, Bonser RS. Biomarkers in acute aortic dissection and other aortic syndromes. J Am Coll Cardiol. 2010; 56:1535–1541.
 XML Download
XML Download