

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Coronary stent deformation is a relatively rare complication of percutaneous coronary intervention. Stent deformation is axial shortening or lengthening of a stent after implantation, resulting from interaction with an ancillary device such as a guide catheter, post-dilatation balloon, or intravascular ultrasound (IVUS) catheter. When the stent deformation protruding to coronary cusp occurs, three therapeutic options can be considered: percutaneous retrieval, surgical removal, or leaving it in-situ. We report a patient with iatrogenic proximal left main stent deformation protruding to the left coronary cusp, successfully managed by crushing the deformed part of the stent to the coronary sinus.
CASE PRESENTATION
A 52-year-old woman was referred to the emergency department because of new onset resting chest pain aggravated with exercise in substernal area. Electrocardiogram showed T wave inversions from precordial V3 to V6. Transthoracic echocardiography showed ejection fraction of 48~53% with severely hypokinetic mid lateral wall, mid septum, mid to apical anterior wall, apex and apical lateral wall suggesting ischemia in the territory of proximal left anterior descending (LAD) coronary artery.
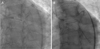
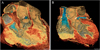
Coronary angiography showed tubular eccentric 90% subtotal stenosis with lesion type (ACC/AHA) B2 in proximal left circumflex artery (LCX), tubular eccentric 75% stenosis with lesion type (ACC/AHA) B2 in mid-LAD and tubular eccentric 90% tandem stenosis with lesion type (ACC/AHA) C in LM ostium to proximal LAD. We deployed Xience Xpedition™ (Abbott, US) 2.75 mm by 18 mm stent at LCX, Xience Xpedition™ 2.75 mm by 18 mm at mid LAD, Xience Xpedition™ 4.0 mm by 33 mm at LM ostium to proximal LAD. After the LM stent implantation, Choice PT wire was used to rewire at LCX, and a Lacrosse 2.5 mm by 15 mm balloon (Goodman Co, Ltd, Sakae, Japan) was forcefully advanced to the LCX ostium. After the balloon dilation to the LCX ostium extending to the proximal LM, we found out that the Choice PT wire undermined the proximal part of the LM stent (Fig. 1A), resulting in deformation of the LM stent, which was left hanging at the left coronary cusp (Fig. 1B). IVUS showed the deformed stent protruding toward the left coronary cusp (Fig. 2A). We tried to crush the deformed part of the LM stent against the left coronary cusp by pushing it with a guiding catheter three times (Fig. 3A, 3B). Follow-up IVUS showed the crushed stent toward the left coronary cusp (Fig. 2B). In order to accurately evaluate the deformed stent, three-dimensional contrast-enhanced coronary CT angiography (Fig. 4A, 4B) was conducted to accurately evaluate the deformed stent. It showed that coronary artery stents in the LM, LAD and LCX were patent. It seemed like the deformed stent was stabilized after stent crushing. After the procedure, the patient didn't complain of any chest pain. Dual antiplatelet agents (aspirin and clopidogrel) were prescribed, and the patient didn't have any cardiovascular events during 6-month follow-up.
DISCUSSION
Coronary stent deformation is a relatively rare but considerable complication of percutaneous coronary intervention. Stent deformation occurs by secondary devices either into or withdrawing back through a stent and by overpressure beyond its ultimate tensile stress limit or stent fatigue.1 Degree of deformation can be partial or complete along the stent body in the length or circumference. Stent deformation is usually discovered with in-stent restenosis, stent thrombosis or rarely embolization of deformed stent and aneurysm, however, it can be incidental finding.
The most iatrogenic stent deformation occurs unintentionally due to partial overloading during deployment. When stent deformation occurs, clinical decision depends on severity of the deformation, hemodynamic instability and functional integrity. At this case, three therapeutic options of the stent deformation are similar those of retained guide-wire.2 Percutaneous retrieval, surgical removal, or leaving the stent in-situ can be considered. The most desirable one is the retrieval of deformed stent depending on the operator's comfort and experience.34567 However, this procedure has some risks such as vessel injury, coronary spasm, new fragmentation, and distal ischemia. Other option is the surgical removal combined with bypass grafting or direct coronary arteriotomy. When the deformed stent is unlikely to cause complications, leaving the stent in-situ and stent crushing can be one of the options.5
In this case, iatrogenic stent deformation occurred after deployment of the LM stent due to the unintentional undermining of the proximal part of the LM stent with subsequent balloon dilatation. Remaining LM stent fully covered the target lesion of LM to proximal LAD, and protruded part of the deformed stent did not disturb coronary artery flow and not cause any other symptoms related to flow insufficiency. We decided not to perform surgical stent removal in the left coronary cusp because she was hemodynamically and functionally stable. We judged that retrieval of the deformed part of the protruded stent had high risks of vessel injury, coronary spasm, new fragmentation, and distal ischemia. To prevent diminished flow by the protruded stent later on and to ensure the hemodynamic stability by preventing possible thrombus formation at the left main ostium later during the follow-up, we decided to crush the protruded deformed part of the stent. The deformed part of the protruded stent was stabilized after stent crushing with guiding catheter. However, the crushed stents had remnant risks of stent thrombosis or embolization. Hence, we should consider follow-up coronary CT angiography or echocardiogram to confirm that no embolization of deformed stent occurs during the follow-up.


 XML Download
XML Download