

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Coronary artery disease (CAD) is still one of the most important causes of death despite significant research into its risk factors and management. Obesity is a known independent risk factor for CAD, and central obesity is a more potent predictor than peripheral obesity.1,2,3,4 Recent studies suggest that the amount of pericardial fat is correlated with abdominal visceral fat as a marker of central obesity, and pericardial fat has been investigated as a risk factor for CAD.5,6
Coronary computed tomographic angiography (CCTA) can directly show the coronary artery lumen and vessel wall, and has an added strength of quantifying atherosclerotic plaque.7 With recent advances in CCTA imaging techniques, image resolution is much improved despite lower radiation exposure. This leads to increasing CCTA use for the risk stratification or diagnosis of CAD in real-world practice.7,8 However, there has been limited study regarding the correlation between pericardial fat as measured by CCTA and abdominal fat or CAD, especially in patients presenting with chest pain at an outpatient clinic. Therefore, we proposed that the volume of pericardial adipose tissue was different between patients with CAD and patients without CAD, and sought to determine which index of abdominal adiposity best correlated with the volume of pericardial adipose tissue (PAT).
MATERIALS AND METHODS
1. Study population
Participants were examined using CCTA between October 2007 and January 2008 at Samsung Medical Center in Seoul. All participants visited an outpatient clinic and had no previous history of CAD. Of the 237 participants, two patients were excluded for their foreigner status. Thirty-three patients were excluded for having unsuitable CCTA to evaluate pericardial fat because their study did not include a non-contrast images or pulmonary artery trunk. An additional 13 patients were excluded for previously performed percutaneous coronary intervention or coronary artery bypass grafting. Participants were classified into groups of patients with CAD and patients without CAD. CAD was defined by CCTA. Baseline clinical characteristics and laboratory data were obtained from medical records and telephone interview, if necessary.
2. Study design
Patients underwent CCTA using a 64-slice multidetector-row scanner (Aquilion 64, Toshiba Medical Systems, Tokyo, Japan) in the supine position. An oral beta-blocker (metoprolol) was used for patients with heart rates >65 beats/min and nitroglycerin for all patients unless contraindicated. The scanning parameters were set to 120 kV, 400 mAs, 64×0.5 mm collimation, 0.4-mm increment, and 0.4-s tube rotation time. A biphasic intravenous contrast injection protocol was used, and it consisted of 65 mL of nonionic contrast medium (iomeprol, 350 mg/mL, Bracco, Milan, Italy) at a flow rate of 4 mL/s followed by 30 mL of mixed normal saline (70%) and contrast medium (30%) at a rate of 3 mL/s. The image was reconstructed with retrospective electrocardiographic gating. Reconstructed slice thickness was 0.625 mm with a slice overlap of 33%. In addition, two slices of 5 mm in thickness were obtained at the level of the umbilicus before taking CCTA.
A dedicated workstation (GE Advantage Workstation 4.3, GE Healthcare, Milwaukee, WI, USA) was used for analysis of coronary artery stenosis. CAD was defined as 50% or more stenosis of main epicardial coronary arteries. A coronary artery calcium score was also measured from the non-contrast images using a method previously described by Agatston et al.9 PAT volume was measured using commercial software (Terarecon Intuition, version 4.4.7, TeraRecon Inc., Foster City, CA, USA). To determine adipose tissue, a predefined image display setting based on Hounsfield units (HU) was used (window width, -150 to -50 HU). PAT was determined by manual tracing of a single region of interest at the pericardium on each slice (Fig. 1). The volume of PAT was calculated using the sum of each slice's PAT area from the cardiac apex to bifurcation of the main pulmonary artery. Enhanced images of the coronary arteries were masked prior to pericardial fat measurement in order to avoid potential bias.
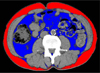
Using a dedicated offline workstation (Virtual Place, AZE Inc., Tokyo, Japan), the abdominal adipose tissue areas and waist circumference in each subject were determined from images taken at the level of the umbilicus. The adipose tissue areas were calculated by automatic planimetry. Waist circumference was determined using a mobile caliper.10 Abdominal visceral adipose tissue (AVAT) area was defined as intraperitoneal fat, with attenuation ranging from -150 to -50 HU. Extraperitoneal fat between the skin and muscles with the same density as AVAT was defined as the abdominal subcutaneous adipose tissue (ASAT) area (Fig. 2). The abdominal total adipose tissue (ATAT) area was a sum of AVAT area and ASAT area.
3. Statistical analysis
Continuous variables were expressed as mean±standard deviation or median and interquartile range, and were compared using the independent t-test or Mann-Whitney U-test, as appropriate. Categorical variables were compared with Pearson's χ2 or Fisher's exact tests. Pearson correlation analyses between PAT and adiposity traits also were performed. Multivariable logistic regression analysis was performed with the enter method to determine the independent predictors of CAD. Covariates included age, sex, hypertension, diabetes mellitus, dyslipidemia, current smoker, typical chest pain, PAT, AVAT, and coronary artery calcium score. A value of p<0.05 in the two-tailed test was considered significant. All analyses were performed with PASW Statistics software version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
1. Baseline clinical characteristics of the study population
A total of 189 patients were included. The mean participant age was 57.7±9.9 years (range, 24 to 85 years), and 106 (56.1%) patients were male. Mean height, weight, and body mass index (BMI) were 162.6±8.3 cm, 66.5±10.7 kg, and 25.1±3.3 kg/m2, respectively. The prevalence of hypertension, diabetes mellitus, cerebrovascular accidents, and dyslipidemia were 43.4%, 27.0%, 3.2%, and 41.3%, respectively. Thirty patients (15.9%) were current smokers. The reason for performing CCTA was typical chest pain in 21 patients (11.1%), atypical chest pain in 142 patients (75.1%), and unknown in 27 patients (14.7%).
Fifty patients (26.5%) had CAD and 139 patients did not have CAD. Baseline clinical and laboratory characteristics of the participants are shown in Table 1. Patients with CAD were older, male predominant, and had more risk factors for CAD, such as hypertension, diabetes mellitus, and dyslipidemia, than patients without CAD. The proportion of typical chest pain in patients with CAD was higher than in patients without CAD. The level of high density lipoprotein cholesterol in patients with CAD was lower, and the level of N-terminal pro-brain natriuretic peptide in patients with CAD was higher than in patients without CAD.
2. Indices of adiposity measured using CCTA
Mean PAT volume, ATAT area, ASAT area, AVAT area, and abdominal circumference for total participants were 154.4±55.4 cm3, 278.2±88.5 cm2, 144.4±57.0 cm2, 120.3±48.6 cm2, and 98.3±12.3 cm, respectively. PAT volume and PAT volume/BMI in patients with CAD were larger than those in patients without CAD (173.2±64.2 cm3 vs. 147.6±50.4 cm3, p<0.01, and 6.87±2.25 cm3·m2/kg vs. 5.85±1.81 cm3·m2/kg, p<0.01). Indices of abdominal adiposity, however, were not different between the two groups (Table 2). The coronary artery calcium score in patients with CAD was higher than that in patients without CAD (89.2 [0-555.4] vs. 0 [0-8.4], p<0.01).
Using multivariable logistic regression analysis, we investigated the independent predictors for CAD (Table 3). PAT volume and coronary artery calcium score determined by CCTA were independent risk factors for CAD (odds ratio [OR] 1.01, 95% confidence interval [CI] 1.00-1.02, p=0.04 and OR 1.01, 95% CI 1.00-1.01, p<0.01). Typical chest pain also predicted CAD independently (OR 4.88, 95% CI 1.47-16.21, p=0.01). AVAT and other clinical information were not predictive.
PAT volume increased significantly as age, BMI, ATAT, ASAT, AVAT, and abdominal circumference increased (Table 4). PAT volume best correlated with AVAT area (r=0.587, p<0.01) among the indices of abdominal adiposity. The coronary artery calcium score did not correlate with PAT volume.
DISCUSSION
To our knowledge, this is the first study to evaluate PAT and AVAT using CCTA, especially in patients who visited an outpatient clinic with chest pain. The present study demonstrated that patients with CAD, defined using CCTA, showed larger PAT volume than patients without CAD. PAT volume, coronary artery calcium score, and
typical chest pain were independently associated with CAD. Indices of abdominal adiposity, however, did not predict CAD, although AVAT area was correlated with PAT volume.
Abdominal adiposity is a well-known risk factor for atherosclerosis and represented with AVAT. There have been many studies that quantify visceral adiposity because abdominal visceral fat is more highly correlated with atherosclerotic disease than abdominal subcutaneous fat.1,2,3,4 Moreover, pericardial fat is not only risk factor of developing CAD but also contributor to clinical outcome, even in asymptomatic patients.12 The number of studies targeting pericardial fat as a marker of visceral adiposity has increased due to the relative ease of evaluating pericardial fat using echocardiography.5 CCTA use also has increased as imaging techniques to visualize coronary artery lumen and plaque had improved. Recently the use of CCTA to evaluate CAD has become more common and well validated, especially in ruling out CAD in the emergency department.11 Measuring the volume rather than area or depth of pericardial fat using CCTA also is more feasible. Computed tomography can provide a more accurate quantification of PAT because of its higher spatial resolution compared with echocardiography or magnetic resonance imaging.
Many investigators have endeavored to quantify abdominal visceral or pericardial fat in order to estimate CAD.2,5,13 Seo et al. observed that AVAT area and visceral fat-to-thigh fat area ratio measured with computed tomography were independent risk factors of CAD, although the number of enrolled patients was only one fourth of our participants.2 Patients in their study had CAD confirmed with coronary angiography. Other investigators compared direct measurement of abdominal circumference with computed tomography to quantify visceral adiposity.2,4 Pericardial fat amount measured by multidetector computed tomography was an independent risk factor for stenotic CAD in asymptomatic people.14,15 Our study evaluated patients who visited an outpatient clinic for typical or atypical chest pain, and showed that pericardial fat had predictive power for CAD. We also determined typical chest pain itself was an independent predictor of CAD. This implies history taking is still important in an era of cutting-edge imaging technology.
CCTA-measured PAT volume was an independent predictor of CAD in our study. However, AVAT area was not. This finding might imply that PAT has more important role to develop coronary atherosclerosis than AVAT though paracrine effect. Previous studies support that pericardial fat, as a local visceral fat depot, is associated with CAD and may have a direct effect on pathogenesis of coronary atherosclerosis via a paracrine role.16,17 Earlier results suggested that pericardial fat played a role not only through its source of visceral fat, but also by aggravating vessel wall inflammation or stimulating the progression of coronary atherosclerosis. There have been many studies identifying inflammation as key in the development and progression of atherosclerosis. Several experimental studies demonstrated that pericardial fat was a source of inflammation and could induce CAD.13,18 The proximal distribution of pericardial fat to the epicardial coronary arteries can help to explain the association of PAT volume with increased coronary artery calcium, atherosclerotic plaque, and myocardial ischemia.6,19 High PAT volume showed a positive correlation with a high level of high-sensitivity C-reactive protein and low level of adiponectin in one study, although a difference in the inflammatory marker could not be demonstrated between the two groups.14,20
AVAT represents central obesity and is more powerful risk factor for CAD than ASAT. In this study, AVAT area of patients with CAD was numerically larger than patients without CAD, although the difference was not statistically significant. If more participants were enrolled, the difference might be significant. We showed that AVAT area (r=0.59, p<0.01) was more related to PAT volume than ASAT area (r=0.23, p<0.01), which could explain that AVAT and PAT had similar visceral locations and relationship with various metabolic risk factors. Several studies have shown that PAT volume is highly correlated with coronary atherosclerosis and AVAT volume or area, rather than waist circumference or BMI.14,21,22 However, participants of those studies were asymptomatic patients, while participants of our study complained of chest pain.
There are benefits to using CCTA as the measuring modality. CCTA can directly visualize the coronary artery and has an additional advantage of quantifying or characterizing atherosclerotic plaque.7 CCTA also provides reliable information about the presence and degree of stenotic lesions, pericardial fat, and coronary artery calcification, which are all related to cardiovascular disease.8,14 We also demonstrated that coronary artery calcium score was an independent predictor of CAD, although evaluation of coronary plaque burden was not performed. PAT volume and these additional information obtained from CCTA might be used to defer invasive coronary angiography and intervention or improve cardiovascular events.
This study has several limitations. First, we used a non-randomized, observational study design, which might have unrecognized confounding factors. Although we performed multivariable analysis to adjust for potential confounding factors, we were not able to correct for unmeasured variables. Second, the sample size was too small to show differences in abdominal adiposity between the two groups, although a numerical trend was evident. AVAT area, which is a known predictor of cardiovascular disease, could potentially be identified as a risk factor for CAD if more patients were studied. Traditional risk factors such as age, diabetes, and hypertension are in the same case. Third, a possible selection bias exists because patients who underwent CCTA had presented for a variety of reasons, such as typical chest pain or CAD screening. In addition, the decision to perform CCTA was dependent on the practicing physician's preference. Much information regarding the clinical impact of pericardial fat could be determined if the study were designed for a specific patients group, such as for those with typical chest pain or patients with diabetes mellitus. However, this study has added strength due to our exclusion of patients with a history of CAD. Fourth, we defined CAD as 50% or more stenosis in major epicardial coronary arteries using CCTA. Although CCTA can visualize coronary artery stenosis, its weakness is its predictive value: CCTA has a positive predictive value for CAD as low as 78% and a negative predictive value is high as 98%.7 In addition, CCTA could exaggerate coronary artery stenosis. The designation of 50% stenosis may not be functional stenosis which associated with symptoms or ischemia. Finally, we did not evaluated clinical outcome, which can be improved with early diagnosis. Improving CCTA technology or image reconstruction would make measuring pericardial fat volume easier and more precise. Further studies are needed to evaluate the natural course or future cardiovascular accidents in patients with abundant pericardial fat.
In conclusion, the PAT volume and coronary artery calcium score are strongly associated with CAD. PAT volume is also well correlated with the area of AVAT among indices of abdominal adiposity. As PAT volume measurement is relatively easy and feasible even with nonenhanced chest computed tomography, PAT may be a good indicator for CAD risk-stratification in real-world outpatient practice.




 XML Download
XML Download