

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Coronary artery aneurysm is a rare disease characterized by an abnormal dilatation (diameter >50% of the normal adjacent segments) of localized or diffuse portion of the coronary artery. The prevalence has been reported to vary between 0.3% to 4.9% in several large studies.1,2 It is most commonly found in right coronary artery (RCA) and less frequently found in left coronary artery and has been known that the main cause of aneurysm is atherosclerosis in adult population and Kawasaki disease in both children and adolescents.1 Pathophysiology of the media of the blood vessel plays a major role in progression of coronary artery aneurysm2 that eventually leads to myocardial ischemic events, such as coronary artery thrombosis, distal embolization, rupture or vasospasm.3 We experienced a case of ST-segment elevation myocardial infarction due to coronary artery thrombosis after warfarin interruption in a patient with a large coronary aneurysm. Here, we report this case with a review of the pertinent literature.
CASE REPORT
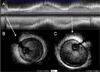
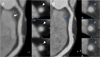
A 44-year-old man, who had a history of myocardial infarction (MI) due to thrombotic occlusion of a large RCA aneurysm 16 months ago (Fig. 1), visited emergency department with acute onset of chest pain. After the first event, he had been received oral anticoagulant (warfarin) in outpatient clinic for 12 months, and then it replaced by aspirin 100 mg just 4 months ago. Since ST-segment elevation was shown in leads II, III and aVF on electrocardiogram (ECG), emergent coronary angiography was performed with a clinical impression of inferior wall MI. Before coronary angiography, we administered clopidogrel 600 mg and intravenous heparin bolus of 5,000 units. Coronary angiography revealed thrombotic total occlusion of RCA with heavy thrombotic burden from middle RCA to the ostium of the posterior descending branch with further enlargement of the aneurysm (Fig. 2A). To dissolve this heavy thrombus, we injected additional intravenous heparin bolus of 5,000 units and intracoronary glycoprotein IIb/IIIa antagonist bolus (abciximab,0.25 mg/kg) and then, we performed mechanic thrombosuction using a 7-Fr thrombosuction catheter (Thrombuster II®, Kaneka Medix, Osaka, Japan) more than 20 times and large amount of red thrombus was aspirated. After aggressive pharmacologic and mechanical treatment, although Thrombolysis in Myocardial Infarction (TIMI) flow was recovered to grade 3, some residual thrombus was still noted on coronary angiography (Fig. 2B). Therefore we have decided to administer additionally intracoronary bolus (3,000 units/kg) of fibrinolytic agent (urokinase) and followed by intravenous continuous infusion (1,000 units/kg) for 12 hours. After urokinase infusion, patient's symptom was completely relieved and ST-segment elevation on ECG was resolved. On hospital day 2, however, the patient complained severe recurrent chest pain accompanied by ST-segment elevation on ECG, and then underwent follow-up coronary angiography that revealed distal embolization of large thrombus to the posterior lateral branch (Fig. 2C), which was similar finding to his first MI event (Fig. 1A and 1B). After mechanical thrombosuction was performed several times with aspiration of large amount of red thrombus, coronary artery flow was fully recovered (TIMI flow grade 3)(Fig. 2D) and when intravascular ultrasound ([IVUS]; Atlantis, Boston Scientific Corporation, Natick, Massachusetts) was performed, atherosclerotic plaque with mild luminal stenosis was shown in proximal RCA and poststenotic dilatation (maximum diameter of 7.5 mm) was observed (Fig. 3). The patient was discharged without any further complications and coronary computed tomography angiography (CCTA) was performed 6 months later that revealed no residual thrombus or further enlargement of aneurysm compared to previous CCTA (Fig. 4). Currently, the patient is receiving life-long anticoagulant therapy with warfarin.
DISCUSSION
Although the precise mechanism leading to the development of aneurysm in the coronary circulation is not well established, genetic predisposition, common risk factors for coronary artery disease, direct vessel injury and abnormal vessel wall metabolism are considered to play important role.1 Atherosclerosis accounts for approximately 50% of all coronary artery aneurysms whether it is by poststenotic dilatation or by direct arterial injury, and Kawasaki disease is the other well-known cause.1,2 In our case, although patient was somewhat young and plaque burden was not so high, when it considered that there was atherosclerotic plaque in proximal RCA and thereafter aneurysmal dilatation was observed distally on CCTA, it would be much proper that atherosclerosis and poststenotic dilatation would be a major pathophysiology of coronary aneurysm which was also confirmed by IVUS and CCTA (Fig. 3 and 4). In Kawasaki disease, similar to atherosclerosis, the main cause of death is also myocardial infarction secondary to thrombosis in aneurysm or stenosis.4
The complication of coronary artery aneurysm may be fatal such as thrombosis or rupture; however the optimal treatment options still remained controversial including anticoagulants, covered stents, reconstruction, resection and exclusion with bypass.5 Our case has shown the therapeutic challenges in patients with large intracoronary thrombus presented with acute myocardial infarction and also embolized distally while treatment. We made every effort to dissolve the heavy thrombus in aneurysm using both pharmacotherapy and mechanical intervention and combination pharmacological regimens contain clopidogrel, intracoronary glycoprotein IIb/IIIa-receptor antagonist (abciximab), intravenous heparin and intracoronary/intravenous thrombolytic agent (urokinase).6,7 There were a small randomized study showed that the intracoronary bolus administration of abciximab in patients undergoing primary PCI was superior to the standard intravenous treatment with respect to infarct size, extent of microvascular obstruction and perfusion8 and a larger-scale randomized trial demonstrated that a low-dose intracoronary administration of streptokinase immediately after primary PCI was effective in significantly limiting long-term infarct size and preserving left ventricular volumes and functions9 and there was a study similar to our case that a direct intracoronary administration of urokinase followed by abciximab treatment significantly reduced the thrombotic burden without increasing the risk of bleeding in 12 patients.10 As we showed in our case, even though we used combined pharmacotherapy including clopidogrel, heparin, abciximab and urokinase, we could not prevent distal embolization. The incidence of distal embolization after percutaneous coronary intervention in patients with large thrombus burden was reported ranges between 6% and 15%.11
Aspirin or warfarin is a common pharmacological treatment to prevent coronary thrombosis or ischemia in patients with coronary aneurysm, however there is a paucity of data and no randomized controlled study to determine their efficacy specifically in coronary aneurysm patients. In our case, it showed that long-term anticoagulation therapy with warfarin rather than aspirin alone would be more effective in patients with large coronary aneurysm who have a past history of distal embolization.
In conclusion, the current case highlights that both combination pharmacotherapy and mechanical intervention would be helpful for the management of patients with acute thrombotic occlusion of large coronary artery aneurysm, and in those patients life-long anticoagulant therapy should be needed to prevent second thromboembolic event.


 XML Download
XML Download