

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Takayasu's arteritis is associated with vascular stenosis involving the aorta, carotid and renal arteries, and pulmonary artery.1 In hypertensive patients due to Takayasu's arteritis, who do not respond to medical treatment, interventional treatment such as angioplasty or surgical treatment such as bypass surgery should be considered. Stent implantation has been reported for the treatment of stenosis of the abdominal aorta and small arteries such as the carotid, mesenteric, or renal arteries in Takayasu's arteritis.1-3
Here, we report a case of successful stent implantation for severe hypertension due to stenosis in the thoracic aorta in a young female patient with Takayasu's arteritis.
CASE REPORT
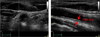
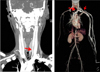
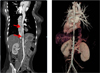
A 21-year-old female came to undergo evaluation for the cause of hypertension which was incidentally detected during health checkup 3 weeks before. The secondary cause of hypertension was not found at the local clinic. On arrival, the patient had a heart rate of 72 beats/min and blood pressure of 150/100 mmHg. On physical examination, a bruit was auscultated over the epigastric area and left neck. Radial arterial pulse was stronger on the right than on the left. In addition, pulses in both femoral, popliteal, dorsalis pedis arteries were weak compared with those in brachial and radial arteries (right arm 150/80 mmHg, left arm 110/70 mmHg, right leg 85/50 mmHg, left leg 80/50 mmHg, respectively). In laboratory tests, erythrocyte sedimentation rate (ESR) to 69 mm/hr and C-reactive protein (CRP) to 1.1 mg/dL. Ankle brachial index (ABI) was 0.53 on the right side and 0.50 on the left side, which suggested the presence of aortic or peripheral arterial disease. In echocardiography, continuous flow was detected in the left common carotid artery and left subclavian artery with increased velocity, which implicated vascular stenosis (Fig. 1). The intima-media thickness (IMT) of the left common carotid artery was 1.94 mm (Fig. 2). In addition, severe stenosis was detected in the transitional area between the descending thoracic aorta and the abdominal aorta (Fig. 3). The peak systolic velocity and the mean pressure gradient were 4.49 m/sec and 80 mmHg, respectively. In neck CT angiography, moderate stenosis was found in the left common carotid artery and in the left subclavian artery (Fig. 4). In chest and abdomen CT angiography, multiple stenotic lesions were detected between the descending thoracic aorta and the abdominal aorta (Fig. 5).
She was diagnosed to have Takayasu's arteritis on the basis of multiple vascular stenosis with no risk factors of cardiovascular diseases, elevated ESR, age and ethnicity (Asian woman). She had no other symptoms associated with vascular stenosis except hypertension. At first, she was treated with corticosteroid in the outpatient department. However, she developed claudication after 2 months. Aortogram showed diffuse stenosis in left common carotid artery and left subclavian artery, but distal run-off was maintained. Between the descending thoracic aorta and the abdominal aorta, long diffuse stenosis was observed and the pressure gradient was 80 mmHg, which was thought to be the cause of claudication. Because medical treatment did not reduce or improve disease progression, percutaneous intervention was performed using a 18×100 mm Nitinol® stent (all in one type, 12 French, Johnson & Johnson) (Fig. 6). After the intervention, the pressure gradient decreased from 80 mmHg to 18 mmHg and her claudication improved. Follow-up CT angiogram 2 days after stent-graft implantation showed patent aorta lumen and good distal flow (Fig. 7). Her blood pressure was normalized with single anti-hypertensive medication and clinical course was uneventful during five-year clinical follow-up.
DISCUSSION
In the case of Takayasu's arteritis with vascular stenosis which does not respond to medical therapy, interventional treatment such as angioplasty or surgical treatment such as bypass surgery should be considered if coronary artery, renal artery or cerebral artery is involved or if ischemia that hinders daily life occurs. Angioplasty has recently been used for treatment along with invasive surgical operations. Surgical bypass of the stenosed segment is often complicated by graft reocclusion, anastomotic site aneurysm and morbidity. Angioplasty offers a less invasive, cost-effective, and safe method for relief of stenotic lesions in patients with Takayasu's arteritis. Stent implantation has been reported for the treatment of stenosis of the abdominal aorta and small arteries such as the carotid, mesenteric, or renal arteries.4-7 Open surgical treatment is currently the gold standard for treating occlusive aortic lesions, yet postoperative morbidity and mortality have remained high.8 On the other hand, endovascular intervention using stenting is less invasive compared to surgical options, resulting in fewer procedural complications and lower mortality.9,10 Good results are seen in the treatment of short focal stenosis in the presence of inactive disease.11,12 The main complications of all intervention, both open surgery and endovascular techniques, include restenosis (75.7%), thrombosis (10%), bleeding (8.6%), and stroke (5.7%).13
In our case, blood pressure was normalized with single anti-hypertensive medication and clinical course was uneventful during five-year clinical follow-up. Secondary hypertension due to aortic stenosis could be managed by a thoracoabdominal endovascular stent in a young female patient with Takayasu's arteritis.




 XML Download
XML Download